外科理论与实践 ›› 2025, Vol. 30 ›› Issue (01): 47-53.doi: 10.16139/j.1007-9610.2025.01.09
李浩1, 骆洋1, 王廷峰2, 林海萍1, 贡婷月1, 赵永恒1, 钟鸣1( )
)
收稿日期:2024-04-02
出版日期:2025-01-25
发布日期:2025-04-25
通讯作者:
钟鸣,E-mail: drzhongming1966@163.com基金资助:
LI Hao1, LUO Yang1, WANG Tingfeng2, LIN Haiping1, GONG Tingyue1, ZHAO Yongheng1, ZHONG Ming1()
Received:2024-04-02
Online:2025-01-25
Published:2025-04-25
摘要:
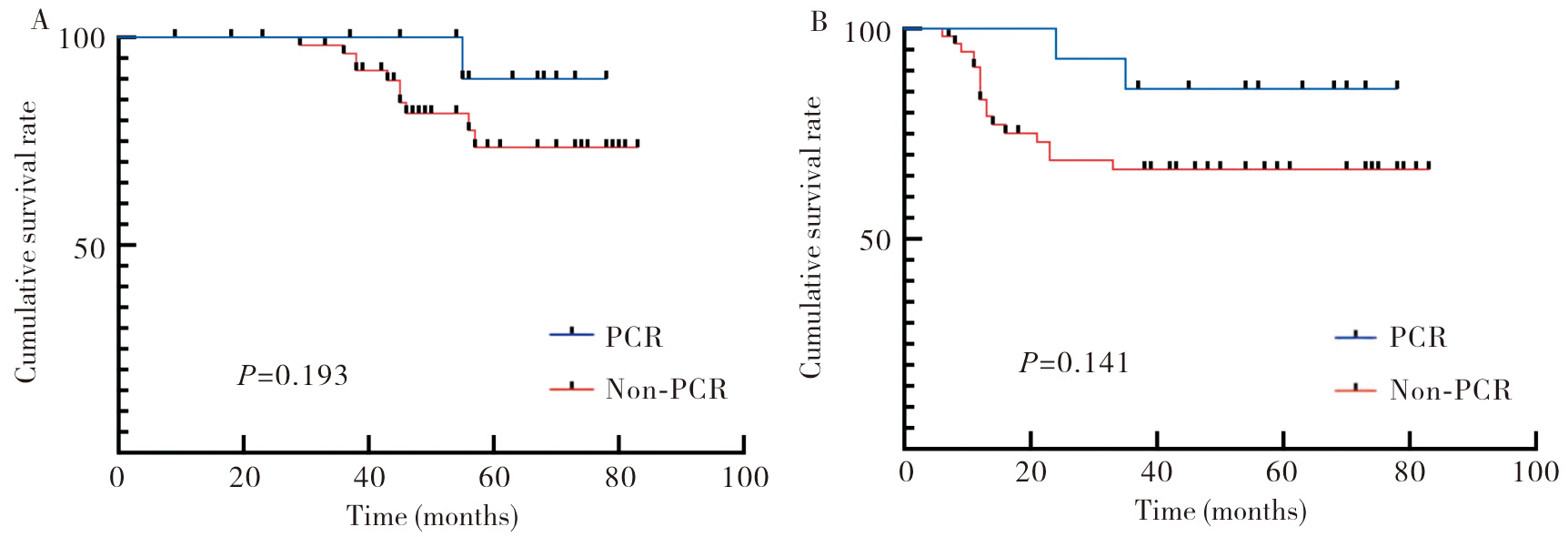
目的: 分析接受新辅助放化疗(nCRT)后行腹腔镜直肠癌根治术的病人中实现病理完全缓解(pCR)的肿瘤特征以及肿瘤预后情况。方法: 回顾性收集2017年1月至2024年1月在仁济医院接受nCRT治疗的局部进展期直肠癌(LARC)病人的临床病理资料。分析影响实现pCR的因素,并比较pCR组与non-pCR组病人预后情况。结果: 单因素分析、多因素Logistic回归分析以及受试者工作特征(ROC)曲线分析显示,肿瘤长径<5 cm(截断值为5.24 cm)和基线癌胚抗原(CEA)<5 μg/L(截断值为5.33 μg/L)是nCRT后实现pCR的独立预测因素。预后生存分析表明,pCR组和non-pCR组的3年总生存(OS)率分别为92.86%和82.46%(P=0.193),3年无病生存(DFS)率分别为85.71%和70.18%(P=0.141),差异均无统计学意义。结论: 肿瘤长径以及基线CEA可作为LARC病人nCRT后实现pCR的独立预测因素。此外,pCR组3年OS和DFS与non-pCR组差异无统计学意义。
中图分类号:
李浩, 骆洋, 王廷峰, 林海萍, 贡婷月, 赵永恒, 钟鸣. 局部进展期直肠癌新辅助治疗后病理完全缓解的预测因素[J]. 外科理论与实践, 2025, 30(01): 47-53.
LI Hao, LUO Yang, WANG Tingfeng, LIN Haiping, GONG Tingyue, ZHAO Yongheng, ZHONG Ming. Predictive factors of pathological complete response after neoadjuvant therapy for locally advanced rectal cancer[J]. Journal of Surgery Concepts & Practice, 2025, 30(01): 47-53.
表1
临床特征[n(%)]
| Characteristics | Total(n=131) | pCR (n=24) | Non-pCR (n=107) | P value |
|---|---|---|---|---|
| Age (years) | 0.154 | |||
| <60 | 54 (41.22) | 13 (54.17) | 41 (38.32) | |
| ≥60 | 77 (58.78) | 11 (45.83) | 66 (61.68) | |
| Gender | 0.088 | |||
| Male | 104 (79.39) | 16 (66.67) | 88 (82.24) | |
| Female | 27 (20.61) | 8 (33.33) | 19 (17.76) | |
| BMI(kg/m2) | 0.303 | |||
| <24 | 103 (78.63) | 17 (70.83) | 86 (80.37) | |
| ≥24 | 28 (21.37) | 7 (29.17) | 21 (19.63) | |
| Baseline T stage | 0.673 | |||
| T3 | 55 (41.98) | 11 (45.83) | 44 (41.12) | |
| T4 | 76 (58.02) | 13 (54.17) | 63 (58.88) | |
| Baseline N stage | 0.895 | |||
| N0 | 23 (17.56) | 5 (20.83) | 18 (16.82) | |
| N1 | 29 (22.14) | 5 (20.83) | 24 (22.43) | |
| N3 | 79 (60.31) | 14 (58.33) | 65 (60.75) | |
| Distance between tumor and anal border (cm) | 0.111 | |||
| <5 | 47 (35.88) | 12 (50.00) | 35 (32.71) | |
| ≥5 | 84 (64.12) | 12 (50.00) | 72 (67.29) | |
| Tumor length (cm) | 0.015 | |||
| <5 | 58 (44.27) | 16 (66.67) | 42 (39.25) | |
| ≥5 | 73 (55.73) | 8 (33.33) | 65 (60.75) | |
| Proportion of tumor in enteric cavity | 0.049 | |||
| ≤1/2 | 48 (36.64) | 13 (54.17) | 35 (32.71) | |
| >1/2 | 83 (63.36) | 11 (45.83) | 72 (67.29) | |
| Baseline CEA level (μg/L) | 0.024 | |||
| <5 | 55 (41.98) | 15 (62.50) | 40 (37.38) | |
| ≥5 | 76 (58.02) | 9 (37.50) | 67 (62.62) | |
| Baseline CA19-9 level (kU/L) | 0.280 | |||
| <27 | 73 (55.73) | 11 (45.83) | 62 (57.94) | |
| ≥27 | 58 (44.27) | 13 (54.17) | 45 (42.06) | |
| Preoperative CEA level (μg/L) | 0.077 | |||
| <5 | 99 (75.57) | 22 (91.67) | 77 (71.76) | |
| ≥5 | 32 (24.43) | 2 (8.33) | 30 (28.04) | |
| Preoperative CA19-9 level (kU/L) | 0.205 | |||
| <27 | 114 (87.02) | 19 (79.17) | 95 (88.79) | |
| ≥27 | 17 (12.98) | 5 (20.83) | 12 (11.21) | |
| Operation | 0.942 | |||
| Low anterior resection | 99 (75.57) | 18 (75.00) | 81 (75.70) | |
| Abdominoperineal resection | 32 (24.43) | 6 (25.00) | 26 (24.30) | |
| Degree of differentiation | 0.387 | |||
| Poorly | 19 (14.50) | 4 (16.67) | 15 (14.02) | |
| Moderately | 95 (72.52) | 15 (62.50) | 80 (74.77) | |
| Well | 17 (12.98) | 5 (20.83) | 12 (11.21) |
表2
Logistic 回归分析
| β | SE | Wald | P value | OR(95%CI) | |
|---|---|---|---|---|---|
| Tumor length(cm) | 0.529 | 0.265 9 | 3.955 | 0.047 | 0.347(0.122-0.985) |
| Proportion of tumor in enteric cavity | 0.167 | 0.259 6 | 0.411 | 0.521 | 0.717(0.259-1.983) |
| Baseline CEA level (μg/L) | 0.520 | 0.244 0 | 4.549 | 0.033 | 0.353(0.136-0.919) |

图1
ROC曲线
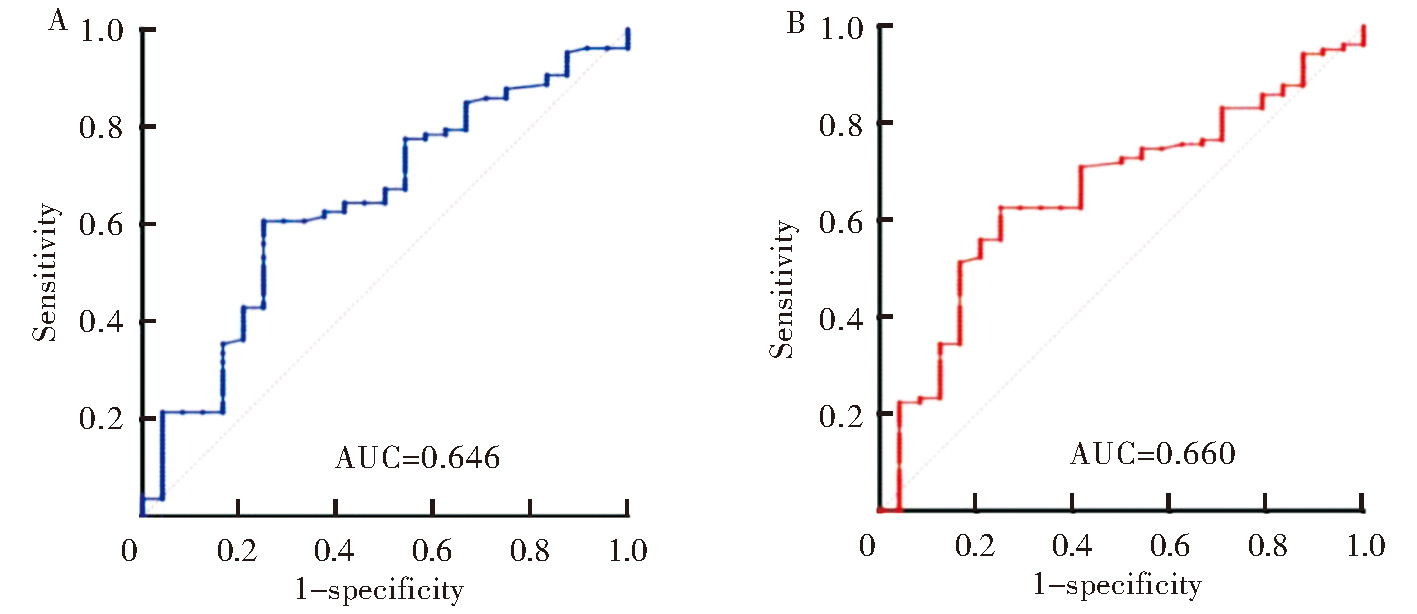

图2
OS和DFS
| [1] |
ARNOLD M, SIERRA M S, LAVERSANNE M, et al. Global patterns and trends in colorectal cancer incidence and mortality[J]. Gut, 2017, 66(4):683-691.
doi: 10.1136/gutjnl-2015-310912 pmid: 26818619 |
| [2] | 元玫雯, 王宏昊, 段如菲, 等. 2016年中国归因于人乳头瘤病毒感染的肿瘤发病与死亡分析[J]. 中华流行病学杂志, 2022, 43(5):702-708. |
|
YUAN M W, WANG H H, DUAN R F, et al. [Analysis on cancer incidence and mortality attributed to human papillomavirus infection in China, 2016][J]. Chin J Epidemiol, 2022, 43(5):702-708.
doi: 10.3760/cma.j.cn112338-20211010-00777 pmid: 35589576 |
|
| [3] | 国家卫生健康委员会医政司, 中华医学会肿瘤学分会. 国家卫健委中国结直肠癌诊疗规范(2023版)[J]. 中国实用外科杂志, 2023, 43(6):602-630. |
| Department of Medical Administration, National Health Comimission; Chinese Society of Oncology. Chinese protocol of diagnosis and treatment of colorectal cancer of the National Health Commission(2023 edition)[J]. Chin J Pract Surg, 2023, 43(6):602-630. | |
| [4] |
PARK I J, YOU Y N, AGARWAL A, et al. Neoadjuvant treatment response as an early response indicator for patients with rectal cancer[J]. J Clin Oncol, 2012, 30(15):1770-1776.
doi: 10.1200/JCO.2011.39.7901 pmid: 22493423 |
| [5] |
MAAS M, NELEMANS P J, VALENTINI V, et al. Long-term outcome in patients with a pathological complete response after chemoradiation for rectal cancer: a pooled analysis of individual patient data[J]. Lancet Oncol, 2010, 11(9):835-844.
doi: 10.1016/S1470-2045(10)70172-8 pmid: 20692872 |
| [6] | ARBMAN G, NILSSON E, HALLBÖÖK O, et al. Local recurrence following total mesorectal excision for rectal cancer[J]. Br J Surg, 1996, 83(3):375-379. |
| [7] |
PAUN B C, CASSIE S, MACLEAN A R, et al. Postoperative complications following surgery for rectal cancer[J]. Ann Surg, 2010, 251(5):807-818.
doi: 10.1097/SLA.0b013e3181dae4ed pmid: 20395841 |
| [8] | GRASS J K, PERSIANI R, TIRELLI F, et al. Robotic versus transanal total mesorectal excision in sexual, anorectal, and urinary function: a multicenter, prospective, observational study[J]. Int J Colorectal Dis, 2021, 36(12):2749-2761. |
| [9] |
CELENTANO V, COHEN R, WARUSAVITARNE J, et al. Sexual dysfunction following rectal cancer surgery[J]. Int J Colorectal Dis, 2017, 32(11):1523-1530.
doi: 10.1007/s00384-017-2826-4 pmid: 28497404 |
| [10] |
LI Y, WANG J, MA X, et al. A review of neoadjuvant chemoradiotherapy for locally advanced rectal cancer[J]. Int J Biol Sci, 2016, 12(8):1022-1031.
doi: 10.7150/ijbs.15438 pmid: 27489505 |
| [11] | HABR-GAMA A, SÃO JULIÃO G P, GAMA-RODRIGUES J, et al. Baseline T classification predicts early tumor regrowth after nonoperative management in distal rectal cancer after extended neoadjuvant chemoradiation and initial complete clinical response[J]. Dis Colon Rectum, 2017, 60(6):586-594. |
| [12] | SANGHERA P, WONG D W, MCCONKEY C C, et al. Chemoradiotherapy for rectal cancer: an updated analysis of factors affecting pathological response[J]. Clin Oncol (R Coll Radiol), 2008, 20(2):176-183. |
| [13] |
SHIN J K, HUH J W, LEE W Y, et al. Clinical prediction model of pathological response following neoadjuvant chemoradiotherapy for rectal cancer[J]. Sci Rep, 2022, 12(1):7145.
doi: 10.1038/s41598-022-10974-7 pmid: 35504888 |
| [14] | 李金娜, 谢凤, 王颖. 局部进展期直肠癌新辅助化疗后病理完全缓解及肿瘤降期的预测因素分析[J]. 现代肿瘤医学, 2021, 29(18):3246-3251. |
| LI J N, XIE F, WANG Y. Predictive factors associated with pathologic complete response and tumor downstaging after neoadjuvant chemotherapy in locally advanced rectal cancer[J]. J Mod Oncol, 2021, 29(18):3246-3251. | |
| [15] | MOUREAU-ZABOTTO L, FARNAULT B, DE CHAISEMARTIN C, et al. Predictive factors of tumor response after neoadjuvant chemoradiation for locally advanced rectal cancer[J]. Int J Radiat Oncol Biol Phys, 2011, 80(2):483-491. |
| [16] | HUANG Y, LEE D, YOUNG C. Predictors for complete pathological response for stage Ⅱ and Ⅲ rectal cancer following neoadjuvant therapy - a systematic review and meta-analysis[J]. Am J Surg, 2020, 220(2):300-308. |
| [17] |
YAN H, WANG R, ZHU K, et al. Predictors of sensitivity to preoperative chemoradiotherapy of rectal adenocarcinoma[J]. Tumori, 2011, 97(6):717-723.
doi: 10.1700/1018.11087 pmid: 22322837 |
| [18] |
DAS P, SKIBBER J M, RODRIGUEZ-BIGAS M A, et al. Predictors of tumor response and downstaging in patients who receive preoperative chemoradiation for rectal cancer[J]. Cancer, 2007, 109(9):1750-1755.
doi: 10.1002/cncr.22625 pmid: 17387743 |
| [19] | YANG K L, YANG S H, LIANG W Y, et al. Carcinoembryonic antigen (CEA) level, CEA ratio, and treatment outcome of rectal cancer patients receiving pre-operative chemoradiation and surgery[J]. Radiat Oncol, 2013,8:43. |
| [20] | YEO S G, KIM D Y, CHANG H J, et al. Reappraisal of pretreatment carcinoembryonic antigen in patients with rectal cancer receiving preoperative chemoradiotherapy[J]. Tumori, 2013, 99(1):93-99. |
| [21] | KANG J H, KIM Y C, KIM H, et al. Tumor volume changes assessed by three-dimensional magnetic resonance volumetry in rectal cancer patients after preoperative chemoradiation: the impact of the volume reduction ratio on the prediction of pathologic complete response[J]. Int J Radiat Oncol Biol Phys, 2010, 76(4):1018-1025. |
| [22] |
HUH J W, KIM H R, KIM Y J. Clinical prediction of pathological complete response after preoperative chemoradiotherapy for rectal cancer[J]. Dis Colon Rectum, 2013, 56(6):698-703.
doi: 10.1097/DCR.0b013e3182837e5b pmid: 23652742 |
| [23] | HIOTIS S P, WEBER S M, COHEN A M, et al. Assessing the predictive value of clinical complete response to neoadjuvant therapy for rectal cancer: an analysis of 488 patients[J]. J Am Coll Surg, 2002, 194(2):131-135;discussion135-136. |
| [24] |
GUILLEM J G, CHESSIN D B, SHIA J, et al. Clinical examination following preoperative chemoradiation for rectal cancer is not a reliable surrogate end point[J]. J Clin Oncol, 2005, 23(15):3475-3479.
pmid: 15908656 |
| [25] | HABR-GAMA A, SÃO JULIÃO G P, VAILATI B B, et al. Organ preservation in cT2N0 rectal cancer after neoadjuvant chemoradiation therapy: the impact of radiation therapy dose-escalation and consolidation chemotherapy[J]. Ann Surg, 2019, 269(1):102-107. |
| [26] | HABR-GAMA A, PEREZ R O, NADALIN W, et al. Operative versus nonoperative treatment for stage 0 distal rectal cancer following chemoradiation therapy: long-term results[J]. Ann Surg, 2004, 240(4):711-717;discussion717-718. |
| [27] |
MAAS M, BEETS-TAN R G, LAMBREGTS D M, et al. Wait-and-see policy for clinical complete responders after chemoradiation for rectal cancer[J]. J Clin Oncol, 2011, 29(35):4633-4640.
doi: 10.1200/JCO.2011.37.7176 pmid: 22067400 |
| [28] | 中国直肠癌新辅助治疗后等待观察数据库研究协作组, 中国医师协会外科医师分会中国医师协会肛肠医师分会, 中华医学会外科学分会结直肠外科学组, 等. 直肠癌新辅助治疗后等待观察策略专家共识(2020版)[J]. 中华胃肠外科杂志, 2020, 23(1):1-9. |
| Chinese Watch & Wait Database Research Cooperation Group(CWWD); Chinese Association of Surgeons, Chinese Society of Coloproctology, Chinese Medical Doctor Association; Chinese Society of Colorectal Surgery, Chinese Medical Association, et al. [Consensus on the Watch and Wait policy in rectal cancer patients after neoadjuvant treatment (2020 version)][J]. Chin J Gastrointest Surg, 2020, 23(1):1-9. |
| [1] | 王甜, 杨敏利. 唇腭裂术前呼吸道感染及手术预后相关影响因素与预测模型构建[J]. 组织工程与重建外科杂志, 2025, 21(1): 40-. |
| [2] | 张俊花, 李一林, 谢静远, 张春丽, 徐静. C3肾病临床预后相关病理特征分析[J]. 诊断学理论与实践, 2024, 23(06): 587-593. |
| [3] | 张煜, 查晴, 杨玲, 叶佳雯, 杨克, 刘艳. 血清MG53水平与冠状动脉钙化的相关性研究[J]. 内科理论与实践, 2024, 19(05): 303-309. |
| [4] | 王虹晓, 苏琪莹, 阎骅. 结直肠癌预后生物标志物研究进展[J]. 内科理论与实践, 2024, 19(05): 337-341. |
| [5] | 阮淼, 笪倩, 许海敏, 董磊, 费晓春. HER2低表达乳腺癌临床病理学特征及预后研究[J]. 诊断学理论与实践, 2024, 23(05): 500-508. |
| [6] | 王玉蓉, 汪元元, 翁海燕. 胃肠道平滑肌肉瘤临床病理分析3例报告[J]. 诊断学理论与实践, 2024, 23(05): 537-541. |
| [7] | 李卓含, 黄新韵, 郭睿, 李彪. 18F-FDG PET/CT在滤泡性淋巴瘤诊断和预后评估中的研究进展[J]. 诊断学理论与实践, 2024, 23(04): 439-444. |
| [8] | 朱维维, 李倩, 吴凡, 翟志敏. 100例骨髓增生异常性肿瘤患者基因突变及其与临床特征间的关系[J]. 诊断学理论与实践, 2024, 23(03): 305-312. |
| [9] | 王雅琪, 夏凡, 章真. 局部进展期直肠癌新辅助放化疗联合免疫治疗的回顾和展望[J]. 外科理论与实践, 2024, 29(03): 220-229. |
| [10] | 谢海艇, 胡烨婷, 李军, 丁克峰. 局部进展期直肠癌的手术时机把握[J]. 外科理论与实践, 2024, 29(03): 206-210. |
| [11] | 巩皓, 迟骋, 张晓霞. 外周灌注指数联合APACHE Ⅱ评分预测脓毒性休克患者28天预后的价值[J]. 内科理论与实践, 2024, 19(03): 174-179. |
| [12] | 林起柱, 刘红枝, 黄霆峰, 范瑞林, 周伟平, 郑树国, 楼健颖, 曾永毅. 基于肝内胆管癌预后模型筛选辅助化疗受益人群[J]. 外科理论与实践, 2024, 29(02): 170-178. |
| [13] | 宋庆杰, 汤娟娟, 赵健全, 宋辉, 杨军. 高脂血症对乙肝相关肝细胞癌病人预后的影响[J]. 外科理论与实践, 2024, 29(02): 143-147. |
| [14] | 胡彬蔚, 沈柏用. 胰腺癌新辅助治疗的优势和进展[J]. 外科理论与实践, 2024, 29(01): 74-80. |
| [15] | 莫建涛, 曹瑞奇, 任加强, 耿智敏, 仵正, 程亚丽. 意外胆囊癌病人预后列线图模型的构建[J]. 外科理论与实践, 2024, 29(01): 40-45. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||