Journal of Surgery Concepts & Practice ›› 2022, Vol. 27 ›› Issue (03): 221-228.doi: 10.16139/j.1007-9610.2022.03.008
• Original article • Previous Articles Next Articles
YIN Yanjiang, LUO Zhiwen, CHEN Xiao, ZHANG Yefan, HUANG Zhen, ZHAO Hong, ZHAO Jianjun, LI Zhiyu, ZHOU Jianguo, CAI Jianqiang, BI Xinyu( )
)
Received:2021-03-09
Online:2022-06-25
Published:2022-08-03
Contact:
BI Xinyu
E-mail:beexy1971@163.com
CLC Number:
YIN Yanjiang, LUO Zhiwen, CHEN Xiao, ZHANG Yefan, HUANG Zhen, ZHAO Hong, ZHAO Jianjun, LI Zhiyu, ZHOU Jianguo, CAI Jianqiang, BI Xinyu. Relationship between surgical margin and prognosis of patients with intrahepatic cholangiocarcinoma[J]. Journal of Surgery Concepts & Practice, 2022, 27(03): 221-228.
| 临床病理因素 | 病例数 | 临床病理因素 | 病例数 |
|---|---|---|---|
| 年龄 | 57.8±9.2 | 淋巴结清扫数 | 4 |
| 性别 | 阳性淋巴结数 | 1 | |
| 男 | 40(56.3%) | 肿瘤最大径(cm) | 5.5±2.2 |
| 女 | 31(43.7%) | >5 | 35(49.3%) |
| 肝炎史 | ≤5 | 36(50.7%) | |
| 无 | 54(76.1%) | LCSGJa)分期 | |
| 乙型肝炎 | 16(22.5%) | Ⅰ | 31(43.7%) |
| 丙型肝炎 | 1(1.4%) | Ⅱ | 19(26.8%) |
| 肝硬化史 | 12(16.9%) | Ⅲ | 6(8.5%) |
| 胆系疾病史 | Ⅳ | 15(21.1%) | |
| 胆结石 | 8(11.3%) | 手术切缘状态 | |
| 胆囊炎 | 7(9.9%) | R0 | 59(83.1%) |
| 无 | 56(78.9%) | R1 | 12(16.9%) |
| 肿瘤数目 | 切缘距离(cm) | 0.4 | |
| 单发 | 66(93.0%) | 术中出血量(mL) | 200 |
| 多发 | 5(7.0%) | 术中输血 | 45(63.4%) |
| 分化程度 | 术中输液量(mL) | 2 200 | |
| 低 | 37(52.1%) | 手术时间(h) | 3.7±1.3 |
| 中 | 32(45.1%) | 术后发生并发症 | 4(5.6%) |
| 高 | 2(2.8%) | 术后住院时间(d) | 9 |
| 血管侵犯 | 27(38.0%) | CA19-9(U/mL) | 130 |
| 其他器官侵犯 | 6(8.5%) | ALT(U/L) | 28 |
| T | AST(U/L) | 24 | |
| T1 | 34(47.9%) | GGT(U/L) | 54 |
| T2 | 20(28.2%) | AFP(μg/L) | 2.96 |
| T3 | 10(14.1%) | CEA(μg/L) | 2.56 |
| T4 | 7(9.9%) | TBIL(μmol/L) | 11.3 |
| N | ALB(g/L) | 47.1±9.5 | |
| N0 | 59(83.1%) | PT(s) | 12.1±1.7 |
| N1 | 12(16.9%) | 腹腔积液 | |
| AJCC分期 | 无 | 65(91.5%) | |
| Ⅰ | 31(43.7%) | 少量 | 5(7.0%) |
| Ⅱ | 19(26.8%) | 多量 | 1(1.4%) |
| Ⅲ | 19(26.8%) | Child-Pugh分级 | |
| Ⅳ | 2(2.8%) | A | 66(93.0%) |
| 淋巴结清扫 | 45(63.4%) | B | 5(7.0%) |
| 变量 | OS期(月) | RFS期(月) | |||||
|---|---|---|---|---|---|---|---|
| P值 | HR | 95%CI | P值 | HR | 95%CI | ||
| 性别 | 0.872 | 0.953 | (0.533, 1.706) | 0.604 | 0.871 | (0.518, 1.466) | |
| 就诊年龄 | 0.892 | 0.998 | (0.968, 1.029) | 0.957 | 1.001 | (0.974, 1.028) | |
| 肝炎史 | 0.718 | 0.882 | (0.448, 1.739) | 0.952 | 1.019 | (0.563, 1.841) | |
| 肝硬化 | 0.579 | 0.796 | (0.355, 1.782) | 0.799 | 0.915 | (0.461, 1.817) | |
| 胆系疾病 | 0.629 | 0.828 | (0.386, 1.777) | 0.598 | 0.837 | (0.432, 1.621) | |
| 肿瘤数目 | 0.017a) | 1.980 | (1.701, 2.591) | 0.005a) | 1.424 | (0.510, 3.981) | |
| 分化程度 | |||||||
| 低 | |||||||
| 中 | 0.572 | 0.844 | (0.468, 1.521) | 0.413 | 0.801 | (0.471, 1.363) | |
| 高 | 0.794 | 0.766 | (0.104, 5.671) | 0.307 | 2.145 | (0.496, 9.284) | |
| 肿瘤最大径 | 0.039a) | 1.113 | (1.014, 1.256) | 0.322 | 1.058 | (0.947, 1.182) | |
| 其他器官侵犯 | 0.028a) | 2.962 | (1.127, 7.788) | 0.307 | 1.630 | (0.639, 4.162) | |
| 淋巴结转移 | 0.007a) | 2.776 | (1.330, 5.792) | 0.002a) | 3.129 | (1.525, 6.422) | |
| LCSGJ分期 | |||||||
| Ⅰ | |||||||
| Ⅱ | 0.784 | 1.111 | (0.524, 2.335) | 0.147 | 0.610 | (0.313, 1.190) | |
| Ⅲ | 0.202 | 1.946 | (0.700, 5.406) | 0.939 | 1.038 | (0.397, 2.716) | |
| ⅣA、ⅣB | 0.056 | 3.073 | (1.434, 6.582) | 0.054 | 1.945 | (0.988, 3.829) | |
| AJCC分期 | |||||||
| ⅠA、ⅠB | |||||||
| Ⅱ | 0.783 | 1.111 | (0.524, 2.356) | 0.146 | 0.609 | (0.313, 1.188) | |
| ⅢA、ⅢB | 0.008a) | 2.600 | (1.277, 5.291) | 0.207 | 1.490 | (0.802, 2.769) | |
| Ⅳ | 0.207 | 3.752 | (0.480, 9.296) | 0.008a) | 2.929 | (2.233, 5.323) | |
| 血管侵犯 | 0.874 | 0.953 | (0.526, 1.725) | 0.038a) | 1.657 | (1.377, 2.144) | |
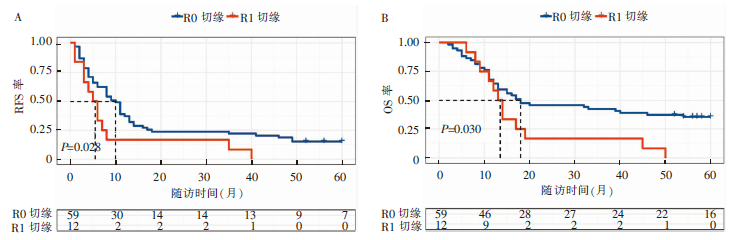
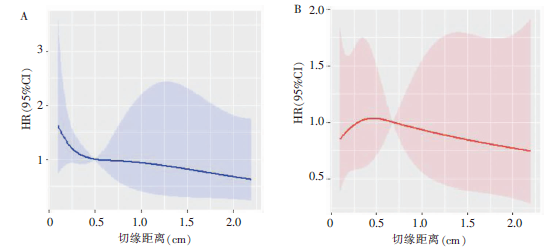
| 手术切缘状态 | 0.008a) | 2.439 | (1.267, 4.696) | 0.011a) | 1.539 | (1.188, 1.894) | |
| ALT | 0.689 | 1.001 | (0.997, 1.004) | 0.987 | 1.000 | (0.996, 1.003) | |
| AST | 0.925 | 1.000 | (0.993, 1.007) | 0.797 | 0.999 | (0.993, 1.005) | |
| GGT | 0.273 | 1.001 | (0.999, 1.003) | 0.046a) | 1.002 | (1.000, 1.003) | |
| AFP | 0.010a) | 1.007 | (1.002, 1.013) | 0.021a) | 1.006 | (1.001, 1.010) | |
| CEA | 0.045a) | 1.005 | (1.000, 1.011) | 0.380 | 1.002 | (0.997, 1.007) | |
| TBIL | 0.243 | 1.003 | (0.998, 1.009) | 0.154 | 1.004 | (0.999, 1.009) | |
| ALB | 0.728 | 1.005 | (0.976, 1.036) | 0.763 | 0.996 | (0.968, 1.024) | |
| PT | 0.424 | 1.067 | (0.911, 1.249) | 0.108 | 1.123 | (0.975, 1.295) | |
| CA19-9 | 0.004a) | 1.768 | (1.198, 2.740) | 0.022a) | 3.377 | (1.507, 5.162) | |
| 腹腔积液 | |||||||
| 无 | |||||||
| 少量 | 0.278 | 0.456 | (0.110, 1.887) | 0.119 | 0.324 | (0.079, 1.337) | |
| 多量 | 0.953 | 0.942 | (0.129, 6.872) | 0.611 | 0.598 | (0.082, 4.352) | |
| Child-Pugh分级 | |||||||
| A | |||||||
| B | 0.328 | 1.595 | (0.626, 4.065) | 0.555 | 1.321 | (0.525, 3.323) | |
| 变量 | OS期(月) | RFS期(月) | |||||
|---|---|---|---|---|---|---|---|
| P值 | HR | 95%CI | P值 | HR | 95%CI | ||
| 肿瘤数目 | 0.123 | 2.463 | (0.783, 7.749) | 0.329 | 1.806 | (0.551, 5.915) | |
| 肿瘤最大直径 | 0.371 | 1.077 | (0.919, 1.255) | ||||
| 其他器官侵犯 | 0.183 | 2.447 | (0.656, 9.135) | ||||
| 淋巴结转移 | 0.474 | 1.514 | (0.487, 4.708) | 0.402 | 1.631 | (0.520, 5.114) | |
| AJCC分期 | |||||||
| ⅠA、ⅠB | |||||||
| Ⅱ | 0.876 | 0.935 | (0.405, 2.158) | 0.686 | 0.811 | (0.293, 2.244) | |
| ⅢA、ⅢB | 0.443 | 1.537 | (0.513, 4.608) | 0.386 | 1.643 | (0.535, 5.040) | |
| Ⅳ | 0.573 | 1.990 | (0.182, 2.779) | 0.026a) | 2.376 | (1.486, 3.375) | |
| 血管侵犯 | 0.242 | 0.586 | (0.239, 1.434) | ||||
| 手术切缘状态 | 0.041a) | 1.946 | (1.438, 2.464) | 0.044a) | 1.582 | (1.011, 2.474) | |
| GGT | 0.301 | 1.001 | (0.999, 1.003) | ||||
| AFP | 0.001a) | 1.010 | (1.004, 1.016) | 0.017a) | 1.006 | (1.001, 1.011) | |
| CEA | 0.847 | 0.999 | (0.991, 1.007) | ||||
| CA19-9 | 0.027a) | 2.310 | (1.263, 3.167) | 0.181 | 1.539 | (0.818, 2.894) | |
| 变量 | R0切缘(n=59) | R1切缘(n=12) | P值 |
|---|---|---|---|
| 年龄(岁) | 57.81 | 57.83 | >0.05 |
| 肝炎史[n(%)] | 43(73) | 11(92) | >0.05 |
| 肝硬化史[n(%)] | 48(81) | 11(92) | >0.05 |
| 胆系疾病史[n(%)] | 47(80) | 10(83) | >0.05 |
| 肿瘤数目(单发/多发)[n(%)] | 57(97)/2(3) | 10(83)/2(17) | <0.05a) |
| 分化程度(低/中、高)[n(%)] | 29(49)/30(51) | 8(67)/4(33) | >0.05 |
| 血管侵犯[n(%)] | 37(63) | 7(58) | >0.05 |
| 其他器官侵犯[n(%)] | 55(93) | 10(83) | >0.05 |
| 肿瘤最大径(cm) | 4.31 | 6.15 | >0.05 |
| AJCC分期(Ⅰ、Ⅱ/Ⅲ、Ⅳ)[n(%)] | 45(76)/14(24) | 5(42)/7(58) | <0.05a) |
| LCSGJ分期(Ⅰ、Ⅱ/Ⅲ、Ⅳ)[n(%)] | 45(76)/14(24) | 5(42)/7(58) | <0.05a) |
| CA19-9(U/mL) | 85.42 | 164.9 | >0.05 |
| ALT(U/L) | 62.95 | 84.75 | >0.05 |
| AST(U/L) | 39 | 52.67 | >0.05 |
| GGT(U/L) | 99.53 | 112.5 | >0.05 |
| AFP(μg/L) | 12.56 | 11.43 | >0.05 |
| CEA(μg/L) | 11.18 | 31.15 | >0.05 |
| TBIL(μmol/L) | 19.62 | 19.93 | >0.05 |
| ALB(g/L) | 45.55 | 44.34 | >0.05 |
| PT(s) | 12.09 | 12.3 | >0.05 |
| 腹腔积液[n(%)] | 54(92) | 11(92) | >0.05 |
| Child-Pugh分级(A/B)[n(%)] | 55(93)/4(7) | 11(92)/1(8) | >0.05 |
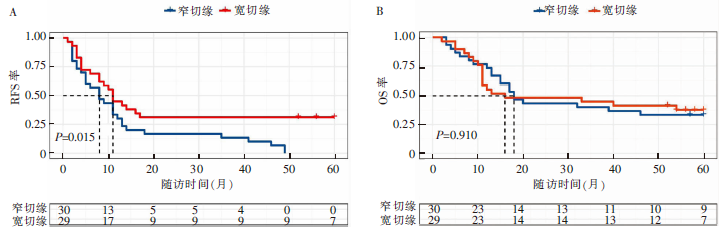
| 变量 | 宽切缘(n=29) | 窄切缘(n=30) | P值 |
|---|---|---|---|
| 术中出血量(mL) | 200.0 | 300.0 | 0.663 |
| 术中输液量(mL) | 2 200.0 | 2 200.0 | 0.673 |
| 手术时间(h) | 3.4±1.3 | 4.0±1.4 | 0.072 |
| 术后住院时间(d) | 8.0 | 9.0 | 0.158 |
| 复发方式[n(%)] | |||
| 肝内 | 13(44.8) | 12(40.0) | 0.911 |
| 肝外 | 16(55.2) | 18(60.0) | |
| 中位RFS期(月) | 11 | 8 | 0.015a) |
| 中位OS期(月) | 18 | 16 | 0.910 |
| [1] | Cillo U, Fondevila C, Donadon M, et al. Surgery for cholangiocarcinoma[J]. Liver Int, 2019, 39 Suppl 1:143-155. |
| [2] |
de Jong MC, Nathan H, Sotiropoulos GC, et al. Intrahe-patic cholangiocarcinoma: an international multi-institutional analysis of prognostic factors and lymph node assessment[J]. J Clin Oncol, 2011, 29(23):3140-3145.
doi: 10.1200/JCO.2011.35.6519 URL |
| [3] |
Watanabe Y, Matsuyama Y, Izumi N, et al. Effect of surgical margin width after R0 resection for intrahepatic cholangiocarcinoma: a nationwide survey of the Liver Cancer Study Group of Japan[J]. Surgery, 2020, 167(5):793-802.
doi: 10.1016/j.surg.2019.12.009 URL |
| [4] |
Chan KM, Tsai CY, Yeh CN, et al. Characterization of intrahepatic cholangiocarcinoma after curative resection: outcome, prognostic factor, and recurrence[J]. BMC gastroenterology, 2018, 18(1):180.
doi: 10.1186/s12876-018-0912-x URL |
| [5] |
Miwa S, Miyagawa S, Kobayashi A, et al. Predictive factors for intrahepatic cholangiocarcinoma recurrence in the liver following surgery[J]. J Gastroenterol, 2006, 41(9):893-900.
doi: 10.1007/s00535-006-1877-z URL |
| [6] |
Fabris L, Cadamuro M, Moserle L, et al. Nuclear expression of S100A4 calcium-binding protein increases cholangiocarcinoma invasiveness and metastasization[J]. Hepatology, 2011, 54(3):890-899.
doi: 10.1002/hep.24466 pmid: 21618579 |
| [7] |
Gerrits PO, Horobin RW, Stokroos I. The effects of glycol methacrylate as a dehydrating agent on the dimensional changes of liver tissue[J]. J Microsc, 1992, 165(Pt 2):273-280.
doi: 10.1111/j.1365-2818.1992.tb01485.x URL |
| [8] |
Riley TR, Ruggiero FM. The effect of processing on liver biopsy core size[J]. Dig Dis Sci, 2008, 53(10):2775-2777.
doi: 10.1007/s10620-007-0181-y URL |
| [9] |
Rutherford EE, Karanjia ND. The measurement of liver resection margins[J]. HPB (Oxford), 2004, 6(1):18-20.
doi: 10.1080/13651820310013402 pmid: 18333039 |
| [10] |
Hanstede JG, Gerrits PO. The effects of embedding in water-soluble plastics on the final dimensions of liver sections[J]. J Microsc, 1983, 131(Pt 1):79-86.
doi: 10.1111/j.1365-2818.1983.tb04233.x URL |
| [11] |
Lang H, Sotiropoulos GC, Sgourakis G, et al. Operations for intrahepatic cholangiocarcinoma: single-institution experience of 158 patients[J]. J Am Coll Surg, 2009, 208(2):218-228.
doi: 10.1016/j.jamcollsurg.2008.10.017 URL |
| [12] |
Lee AJ, Chun YS. Intrahepatic cholangiocarcinoma: the AJCC/UICC 8th edition updates[J]. Chin Clin Oncol, 2018, 7(5):52.
doi: 10.21037/cco.2018.07.03 URL |
| [13] |
Maithel SK, Gamblin TC, Kamel I, et al. Multidisciplinary approaches to intrahepatic cholangiocarcinoma[J]. Cancer, 2013, 119(22):3929-3942.
doi: 10.1002/cncr.28312 URL |
| [14] |
Benson AB, D′Angelica MI, Abbott DE, et al. Guidelines insights: hepatobiliary cancers, version 2.2019[J]. J Natl Compr Canc Netw, 2019, 17(4):302-310.
doi: 10.6004/jnccn.2019.0019 URL |
| [15] |
Rahnemai-Azar AA, Weisbrod AB, Dillhoff M, et al. Intrahepatic cholangiocarcinoma: current management and emerging therapies[J]. Expert Rev Gastroenterol Hepatol, 2017, 11(5):439-449.
doi: 10.1080/17474124.2017.1309290 URL |
| [16] |
Tang H, Lu W, Li B, et al. Influence of surgical margins on overall survival after resection of intrahepatic cholangiocarcinoma: a meta-analysis[J]. Medicine, 2016, 95(35):e4621.
doi: 10.1097/MD.0000000000004621 URL |
| [17] |
Beal EW, Cloyd JM, Pawlik TM. Surgical treatment of intrahepatic cholangiocarcinoma: current and emerging principles[J]. J Clin Med, 2020, 10(1):104.
doi: 10.3390/jcm10010104 URL |
| [18] |
Ma KW, Cheung TT, She WH, et al. The effect of wide resection margin in patients with intrahepatic cholangiocarcinoma: a single-center experience[J]. Medicine, 2016, 95(28):e4133.
doi: 10.1097/MD.0000000000004133 URL |
| [19] |
Spolverato G, Kim Y, Alexandrescu S, et al. Is hepatic resection for large or multifocal intrahepatic cholangiocarcinoma justified? Results from a multi-institutional collaboration[J]. Ann Surg Oncol, 2015, 22(7):2218-2225.
doi: 10.1245/s10434-014-4223-3 pmid: 25354576 |
| [20] | 傅俊, 李俊, 项红军, 等. 肝切除切缘的距离对肝内胆管癌伴乙型肝炎肝硬化预后的影响[J]. 肝胆外科杂志, 2017, 25(2):89-94. |
| [21] |
Farges O, Fuks D, Boleslawski E, et al. Influence of surgical margins on outcome in patients with intrahepatic cholangiocarcinoma: a multicenter study by the AFC-IHCC-2009 study group[J]. Ann Surg,2011, 254(5):824-829.
doi: 10.1097/SLA.0b013e318236c21d URL |
| [22] |
Ribero D, Pinna AD, Guglielmi A, et al. Surgical approach for long-term survival of patients with intrahepatic cholangiocarcinoma: a multi-institutional analysis of 434 patients[J]. Arch Surg, 2012, 147(12):1107-1113.
doi: 10.1001/archsurg.2012.1962 pmid: 22910846 |
| [23] |
Tamandl D, Herberger B, Gruenberger B, et al. Influence of hepatic resection margin on recurrence and survival in intrahepatic cholangiocarcinoma[J]. Ann Surg Oncol, 2008, 15(10):2787-2794.
doi: 10.1245/s10434-008-0081-1 URL |
| [24] |
Bartsch F, Baumgart J, Hoppe-Lotichius M, et al. Intrahepatic cholangiocarcinoma - influence of resection margin and tumor distance to the liver capsule on survival[J]. BMC Surg, 2020, 20(1):61.
doi: 10.1186/s12893-020-00718-7 pmid: 32252724 |
| [25] |
Spolverato G, Yakoob MY, Kim Y, et al. The impact of surgical margin status on long-term outcome after resection for intrahepatic cholangiocarcinoma[J]. Ann Surg Oncol, 2015, 22(12):4020-4028.
doi: 10.1245/s10434-015-4472-9 pmid: 25762481 |
| [26] |
Wang Y, Li J, Xia Y, et al. Prognostic nomogram for intrahepatic cholangiocarcinoma after partial hepatectomy[J]. J Clin Oncol, 2013, 31(9):1188-1195.
doi: 10.1200/JCO.2012.41.5984 URL |
| [27] |
Zhang XF, Bagante F, Chakedis J, et al. Perioperative and long-term outcome for intrahepatic cholangiocarcinoma: impact of major versus minor hepatectomy[J]. J Gastrointest Surg, 2017, 21(11):1841-1850.
doi: 10.1007/s11605-017-3499-6 URL |
| [28] |
Mazzaferro V, Gorgen A, Roayaie S, et al. Liver resection and transplantation for intrahepatic cholangiocarcinoma[J]. J Hepatol, 2020, 72(2):364-377.
doi: S0168-8278(19)30711-1 pmid: 31954498 |
| [29] |
Squires MH, Cloyd JM, Dillhoff M, et al. Challenges of surgical management of intrahepatic cholangiocarcinoma[J]. Expert Rev Gastroenterol Hepatol, 2018, 12(7):671-681.
doi: 10.1080/17474124.2018.1489229 URL |
| [1] | NIE Haihang, WANG Fan, WANG Hongling, ZHAO Qiu. Risk factors and prevention methods for post-ERCP pancreatitis [J]. Journal of Surgery Concepts & Practice, 2023, 28(04): 310-315. |
| [2] | YANG Yi, YANG Xingxia, JIN Sili, ZHANG Xu, ZHU Juanying, CHEN Xiaosong. Clinical application of preoperative MRI examination in breast-conserving surgery for ductal carcinoma in situ [J]. Journal of Surgery Concepts & Practice, 2023, 28(04): 378-382. |
| [3] | YU Lan, ZHANG Yongyi, HUANG Lei, WAN Xin, JIANG Shengyao, TANG Sijing, ZHANG Jun, HU Weiguo. Risk factors of severe postoperative complications in elderly patients with pancreaticoduodenectomy [J]. Journal of Surgery Concepts & Practice, 2023, 28(02): 139-146. |
| [4] | SONG Luqian, CHANG Chunkang. Interpretation of clinical practice guidelines for myelodysplastic syndrome (version 1, 2023) of National Comprehensive Cancer Nerwork(NCCN) [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(02): 116-120. |
| [5] | TAO Yi, MI Jianqing. Interpretation of Multiple Myeloma Guidelines update (version 2, 2023) of National Comprehensive Cancer Network (NCCN) [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(02): 121-126. |
| [6] | QIAO Minjie, ZHOU Wei, CHEN Yi. Role of serum high mobility group box-B1 in evaluating prognosis of sepsis [J]. Journal of Internal Medicine Concepts & Practice, 2023, 18(02): 70-75. |
| [7] | XU Jiankun, ZHOU Luting, ZHANG Wenjing, XU Haimin, WANG Chaofu. The prognostic value of CA9 expression in clear cell renal cell carcinoma [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(01): 37-43. |
| [8] | WANG Han, LU Haidi, WANG Lei, CONG Wenming, ZHENG Jianming, BAI Chenguang. Clinicopathological features of 2 cases of squamous cell carcinoma and 2 cases of adenosquamous carcinoma [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(01): 44-49. |
| [9] | BA Fuhua, ZHONG Ming, CHEN Ying, CHEN Erzhen. Progress in clinical prevention and treatment of refeeding syndrome [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(01): 80-84. |
| [10] |
ZHU Hainan, GU Bin, XIE Feng, et al.
Pre-operation evaluations in vascularized composite tissue allotransplantation [J]. Journal of Tissue Engineering and Reconstructive Surgery, 2022, 18(3): 265-. |
| [11] | WANG Jin, GUO Rui, LI Biao, ZHANG Xiaozhe. Prognostic evaluation of extranodal natural killer/T-cell lymphoma, nasal type(ENKTL) with 18F-FDG PET/CT [J]. Journal of Diagnostics Concepts & Practice, 2022, 21(06): 702-709. |
| [12] | LI Yongde, WANG Yang, LI Xiang, LI Wenjie, XIE Di, JIANG Shaowei, GE Xiaoli, WANG Hairong, GAO Chengjin, PAN Shuming. A retrospective study on prediction of neurological outcome in cardiac arrest patients of out-hospital [J]. Journal of Internal Medicine Concepts & Practice, 2022, 17(06): 447-452. |
| [13] | YANG Cuiyan, WANG Haoyu, CHEN Xiaosong, SHEN Kunwei. Study on tumour suppressor gene TP53 mutation and prognosis in patients with triple-negative breast cancer [J]. Journal of Surgery Concepts & Practice, 2022, 27(05): 421-428. |
| [14] | ZHANG Jixiang, XIE Zhihua, LI Wei, JIANG Xiaoqing. Classification of intrahepatic cholangiocarcinoma and hot topics in surgical treatment [J]. Journal of Surgery Concepts & Practice, 2022, 27(05): 478-482. |
| [15] | XIE Wen, LIANG Huaiyu, DONG Lei, YUAN Fei, WANG Chaofu, GUO Yan. Analysis of genetic status of pivotal driver genes in pancreatic ductal adenocarcinoma and their correlation with clinicopathologic features [J]. Journal of Diagnostics Concepts & Practice, 2022, 21(05): 581-587. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||