诊断学理论与实践 ›› 2023, Vol. 22 ›› Issue (01): 37-43.doi: 10.16150/j.1671-2870.2023.01.006
许建昆, 周露婷, 张文净, 许海敏, 王朝夫( )
)
收稿日期:2022-05-30
出版日期:2023-02-25
发布日期:2023-07-06
通讯作者:
王朝夫
E-mail:wangchaofu@126.com
基金资助:
XU Jiankun, ZHOU Luting, ZHANG Wenjing, XU Haimin, WANG Chaofu()
Received:2022-05-30
Online:2023-02-25
Published:2023-07-06
Contact:
WANG Chaofu
E-mail:wangchaofu@126.com
摘要:
目的: 评估CA9在预测透明细胞肾细胞癌(clear cell renal cell carcinoma, ccRCC)患者术后复发或转移以及生存预后中的价值。方法: 回顾分析上海交通大学医学院附属瑞金医院2017年1月1日至2020年12月31日期间收治的231例ccRCC患者,所有患者均接受了肾癌根治或部分切除术,分析其临床病理资料,并对患者进行随访,统计其肿瘤复发、转移和总生存期(overall survival, OS)、无病生存期(disease-free survival, DFS)情况。收集所有肿瘤组织切片及蜡块,制作组织微阵列,使用CA9多克隆抗体对组织微阵列进行免疫组织化学分析。采用Kaplan-Meier和多元Cox回归模型分析,评估组织微阵列CA9表达水平与患者临床病理特征及OS、DFS间的相关性。结果: 231例ccRCC患者的中位随访时间为37个月(13~54个月),有8例患者死亡,38例(16.5%)患者术后出现肿瘤复发和(或)转移,其中3例出现肿瘤复发,29例发生肿瘤转移,另6例患者同时出现肿瘤复发和肿瘤转移。231例患者中,CA9的阳性表达率为94%(217/231),其中153例(66%) CA9染色率≥85%,78例(34%)CA9染色率<85%。卡方分析显示,CA9的表达不仅与肿瘤T分期、国际泌尿病理学会(International Society of Urological Pathology,ISUP)核分级、肉瘤样或横纹肌样分化(坏死)、被膜侵犯、血管浸润等组织病理学参数相关(P均<0.01),且与肿瘤复发、转移及患者生存状态相关(P均<0.01),但与年龄、性别及肿瘤发生部位无关(P均>0.05)。卡方分析表明,CA9(<85%)低表达是ccRCC患者术后OS、DFS不良的预测因素,危险比分别为6.211(P=0.002)和8.980(P<0.001)。结论: ccRCC组织中CA9低表达与低OS、DFS相关,是ccRCC患者术后短OS和短DFS的独立危险因素,可作为评估ccRCC患者预后的分子标志物。
中图分类号:
许建昆, 周露婷, 张文净, 许海敏, 王朝夫. CA9在透明细胞肾细胞癌预后评估中的价值[J]. 诊断学理论与实践, 2023, 22(01): 37-43.
XU Jiankun, ZHOU Luting, ZHANG Wenjing, XU Haimin, WANG Chaofu. The prognostic value of CA9 expression in clear cell renal cell carcinoma[J]. Journal of Diagnostics Concepts & Practice, 2023, 22(01): 37-43.
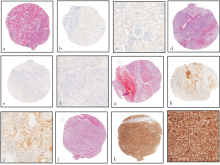
图1
正常肾上皮和透明细胞肾细胞癌ccRCC标本中CA9 HE和IHC染色的代表性图像 正常肾上皮和ccRCC标本中CA9 HE和IHC染色的图像。正常肾组织中CA9普遍呈阴性(a:×10,b:×10,c:×40);CA9在ccRCC组织中阴性表达(d:×10,e:×10,f:×40);CA9在ccRCC组织中<85%表达(g:×10,h:×10,i:×40);CA9在ccRCC组织中≥85%表达(j:×10,k:×10,l:×40)。
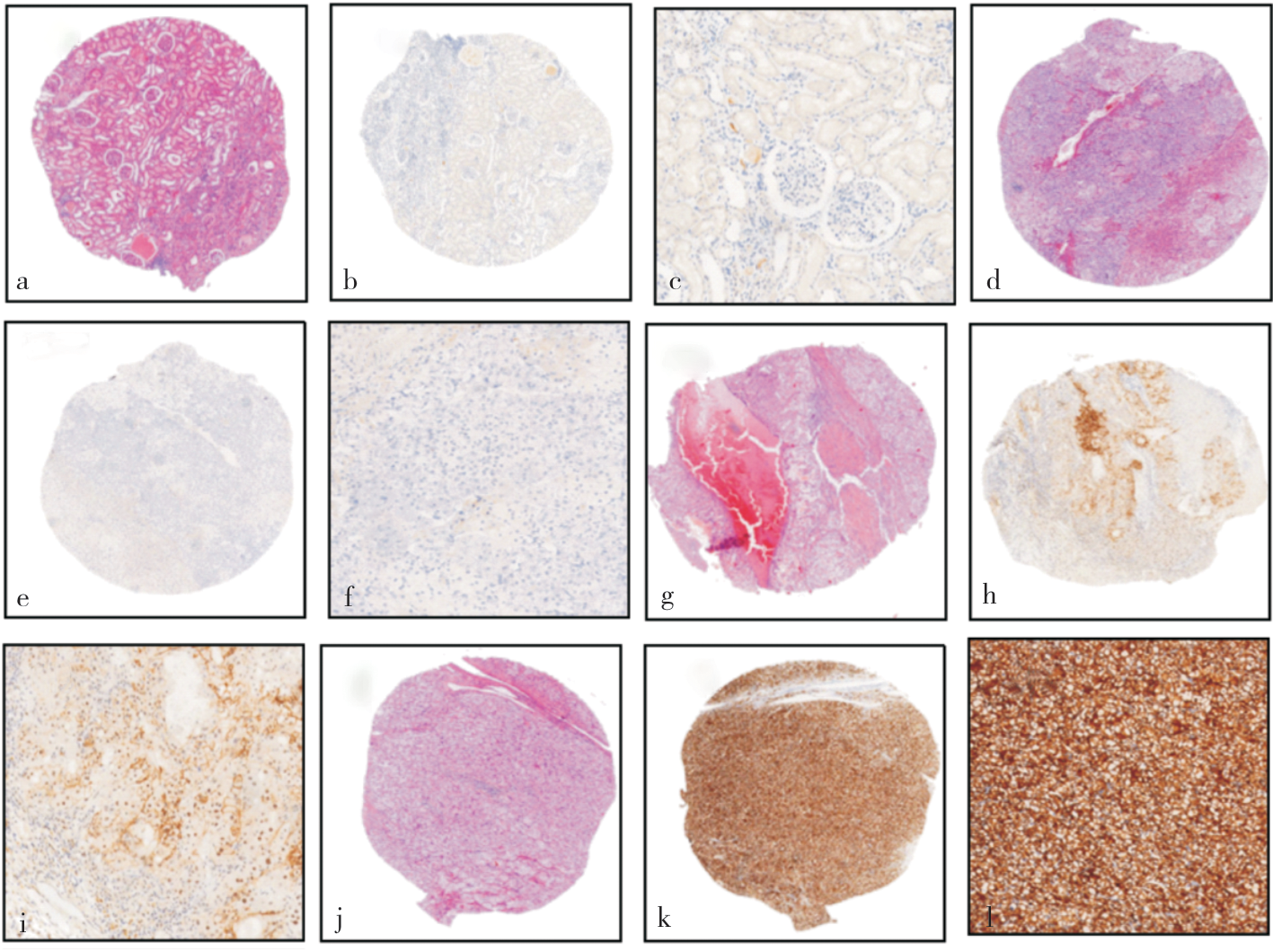
表1
ccRCC患者的临床病理特点(N=231)
| Parameter | Number | Percentage(%) |
|---|---|---|
| Age (years) | ||
| Median | 58 | |
| Range | 20~91 | |
| Gender | ||
| Male | 152 | 65.8 |
| Female | 79 | 34.2 |
| Tumour site | ||
| Left | 118 | 51.1 |
| Right | 113 | 48.9 |
| Furman grade | ||
| 1 | 8 | 3.5 |
| 2 | 148 | 64.0 |
| 3 | 42 | 18.2 |
| 4 | 33 | 14.3 |
| T stage | ||
| Ⅰ | 168 | 72.7 |
| Ⅱ | 22 | 9.5 |
| Ⅲ | 22 | 9.5 |
| Ⅳ | 19 | 8.3 |
| Rhabdoid or sarcomatoid differentiation | ||
| No | 206 | 89.2 |
| Yes | 25 | 10.8 |
| Necrosis | ||
| No | 182 | 78.8 |
| Yes | 49 | 21.2 |
| Capsular invasion | ||
| No | 206 | 89.2 |
| Yes | 25 | 10.5 |
| Vascular invasion | ||
| No | 211 | 91.3 |
| Yes | 20 | 8.7 |
表2
CA9在ccRCC中的表达与临床病理特征的单因素卡方分析
| Parameter | Amount | CA9 expression | P | |
|---|---|---|---|---|
| Negative | Positive | |||
| Age (years) | ||||
| ≤55 | 84 | 26(31.0%) | 58(69.0%) | 0.494 |
| >55 | 147 | 52(35.4%) | 95(64.6%) | |
| Gender | ||||
| Male | 152 | 58(38.2%) | 94(61.8%) | 0.050 |
| Female | 79 | 20(25.3%) | 59(74.7%) | |
| Tumour site | ||||
| Left | 118 | 38(32.2%) | 80(67.8%) | 0.608 |
| Right | 113 | 40(35.4%) | 73(64.6%) | |
| Furman grade | ||||
| 1-2 | 156 | 38(24.4%) | 118(75.6%) | <0.001 |
| 3-4 | 75 | 40(53.3%) | 35(46.7%) | |
| T stage | ||||
| Ⅰ-Ⅱ | 190 | 44(23.2%) | 146(76.8%) | <0.001 |
| Ⅲ-Ⅳ | 41 | 34(82.9%) | 7(17.1%) | |
| Rhabdoid or sarcomatoid differentiation | ||||
| No | 206 | 58(28.2%) | 148(71.8%) | <0.001 |
| Yes | 25 | 20(80.0%) | 5(20.0%) | |
| Necrosis | ||||
| No | 182 | 42(23.1%) | 142(76.9%) | <0.001 |
| Yes | 49 | 36(73.5%) | 13(26.5%) | |
| Capsular invasion | ||||
| No | 206 | 59(28.6%) | 147(71.4%) | <0.001 |
| Yes | 25 | 19(76.0%) | 6(24.0%) | |
| Vascular invasion | ||||
| No | 211 | 61(28.9%) | 150(71.1%) | <0.001 |
| Yes | 20 | 17(85.0%) | 3(15.0%) | |
| Relapse or metastasis | ||||
| No | 193 | 45(23.3%) | 148(76.7%) | <0.001 |
| Yes | 38 | 33(86.8%) | 5(13.2%) | |
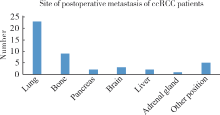
图2
38例ccRCC患者术后转移部位
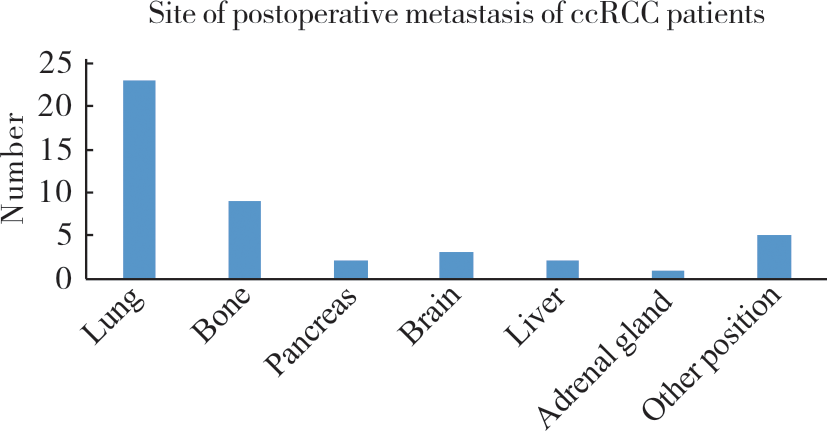
表3
ccRCC患者OS的单因素和多因素分析
| Parameter | Univariate analysis | multivariate analysis | |
|---|---|---|---|
| P | Risk ratio(95%CI) | P | |
| Gender | <0.001 | 0.102(0.013-0.767) | 0.027 |
| Tumour site | 0.235 | ||
| Age(>55 years) | 0.840 | ||
| Furman Grade(3-4) | <0.001 | 0.534(0.165-1.724) | 0.294 |
| Rhabdoid differentiation | <0.001 | 1.106(0.375-3.261) | 0.855 |
| Necrosis | <0.001 | 0.725(0.210-2.500) | 0.610 |
| T Stage(Ⅲ-Ⅳ) | <0.001 | 1.131(0.223-5.730) | 0.882 |
| Capsular invasion | <0.001 | 0.503(0.130-1.944) | 0.319 |
| Vascular invasion | <0.001 | 0.491(0.141-1.710) | 0.264 |
| CA9 low expression | <0.001 | 6.211(1.908-20.00) | 0.002 |
表4
对ccRCC患者DFS的单因素和多因素分析
| Parameter | Univariate analysis | Multivariate analysis | |
|---|---|---|---|
| P | Risk ratio(95%CI) | P | |
| Gender | 0.001 | 0.356(0.123-1.025) | 0.056 |
| Tumour site | 0.483 | ||
| Age(>55 years) | 0.295 | ||
| Furman Grade(3-4) | <0.001 | 0.404(0.159-1.026) | 0.057 |
| Rhabdoid differentiation | <0.001 | 1.040(0.458-2.359) | 0.926 |
| Necrosis | <0.001 | 0.746(0.290-1.920) | 0.543 |
| T Stage(Ⅲ-Ⅳ) | <0.001 | 1.591(0.460-5.511) | 0.464 |
| Capsular invasion | <0.001 | 0.350(0.121-1.011) | 0.052 |
| Vascular invasion | <0.001 | 0.616(0.229-1.658) | 0.337 |
| CA9 low expression | <0.001 | 8.980(3.219~25.057) | <0.001 |
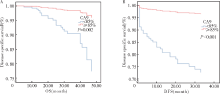
图3
ccRCC患者CA9的表达与OS及DFS间的关系 A: CA9 表达与 OS的相关性;B:CA9表达与DFS的相关性。
| [1] |
HSIEH J J, PURDUE M P, SIGNORETTI S, et al. Renal cell carcinoma[J]. Nat Rev Dis Primers, 2017, 3:17009.
doi: 10.1038/nrdp.2017.9 pmid: 28276433 |
| [2] |
SIEGEL R L, MILLER K D, JEMAL A. Cancer statistics, 2019[J]. CA Cancer J Clin, 2019, 69(1):7-34.
doi: 10.3322/caac.v69.1 URL |
| [3] |
GRAY R E, HARRIS G T. Renal Cell Carcinoma: Diagnosis and Management[J]. Am Fam Physician, 2019, 99(3):179-184.
pmid: 30702258 |
| [4] |
BRAY F, FERLAY J, SOERJOMATARAM I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2018, 68(6):394-424.
doi: 10.3322/caac.v68.6 URL |
| [5] |
COHEN H T, MCGOVERN F J. Renal-cell carcinoma[J]. N Engl J Med, 2005, 353(23):2477-2490.
doi: 10.1056/NEJMra043172 URL |
| [6] |
KROEGER N, ZIMMERMANN U, BURCHARDT M, et al. Prognostication in localised renal cell carcinoma[J]. Lancet Oncol, 2015, 16(6):603-604.
doi: 10.1016/S1470-2045(15)70227-5 pmid: 25979596 |
| [7] |
LEIBOVICH B C, HAN K R, BUI M H, et al. Scoring algorithm to predict survival after nephrectomy and immunotherapy in patients with metastatic renal cell carcinoma: a stratification tool for prospective clinical trials[J]. Cancer, 2003, 98(12):2566-2575.
pmid: 14669275 |
| [8] |
KLATTE T, ROSSI S H, STEWART G D. Prognostic factors and prognostic models for renal cell carcinoma: a lite-rature review[J]. World J Urol, 2018, 36(12):1943-1952.
doi: 10.1007/s00345-018-2309-4 |
| [9] |
RENSHAW A A, CHEVILLE J C. Quantitative tumour necrosis is an independent predictor of overall survival in clear cell renal cell carcinoma[J]. Pathology, 2015, 47(1):34-37.
doi: 10.1097/PAT.0000000000000193 URL |
| [10] |
TSUI K H, SHVARTS O, SMITH R B, et al. Prognostic indicators for renal cell carcinoma: a multivariate analysis of 643 patients using the revised 1997 TNM staging criteria[J]. J Urol, 2000, 163(4):1090-1095.
doi: 10.1016/s0022-5347(05)67699-9 pmid: 10737472 |
| [11] |
LAM J S, LEPPERT J T, FIGLIN R A, et al. Role of molecular markers in the diagnosis and therapy of renal cell carcinoma[J]. Urology, 2005, 66(5 Suppl):1-9.
doi: 10.1016/j.urology.2005.06.112 pmid: 16194700 |
| [12] |
BUI M H, ZISMAN A, PANTUCK A J, et al. Prognostic factors and molecular markers for renal cell carcinoma[J]. Expert Rev Anticancer Ther, 2001, 1(4):565-575.
doi: 10.1586/14737140.1.4.565 URL |
| [13] |
KIM H L, SELIGSON D, LIU X, et al. Using tumor mar-kers to predict the survival of patients with metastatic renal cell carcinoma[J]. J Urol, 2005, 173(5):1496-1501.
doi: 10.1097/01.ju.0000154351.37249.f0 URL |
| [14] |
IVANOV S, LIAO S Y, IVANOVA A, et al. Expression of hypoxia-inducible cell-surface transmembrane carbonic anhydrases in human cancer[J]. Am J Pathol, 2001, 158(3):905-919.
pmid: 11238039 |
| [15] |
MAXWELL P H, WIESENER M S, CHANG G W, et al. The tumour suppressor protein VHL targets hypoxia-inducible factors for oxygen-dependent proteolysis[J]. Nature, 1999, 399(6733):271-275.
doi: 10.1038/20459 URL |
| [16] | BUI M H, SELIGSON D, HAN K R, et al. Carbonic anhydrase Ⅸ is an independent predictor of survival in advanced renal clear cell carcinoma: implications for prognosis and therapy[J]. Clin Cancer Res, 2003, 9(2):802-811. |
| [17] | BENEJ M, PASTOREKOVA S, PASTOREK J. Carbonic anhydrase Ⅸ: regulation and role in cancer[J]. Subcell Biochem, 2014, 75:199-219. |
| [18] | TAFRESHI N K, LLOYD M C, BUI M M, et al. Carbonic anhydrase Ⅸ as an imaging and therapeutic target for tumors and metastases[J]. Subcell Biochem, 2014, 75:221-254. |
| [19] |
ZATOVICOVA M, JELENSKA L, HULIKOVA A, et al. Carbonic anhydrase Ⅸ as an anticancer therapy target: preclinical evaluation of internalizing monoclonal antibody directed to catalytic domain[J]. Curr Pharm Des, 2010, 16(29):3255-3263.
doi: 10.2174/138161210793429832 URL |
| [20] |
ZHAO Z, LIAO G, LI Y, et al. Prognostic value of carbonic anhydrase Ⅸ immunohistochemical expression in renal cell carcinoma: a meta-analysis of the literature[J]. PLoS One, 2014, 9(11):e114096.
doi: 10.1371/journal.pone.0114096 URL |
| [21] |
LEIBOVICH B C, SHEININ Y, LOHSE C M, et al. Carbonic anhydrase Ⅸ is not an independent predictor of outcome for patients with clear cell renal cell carcinoma[J]. J Clin Oncol, 2007, 25(30):4757-4764.
doi: 10.1200/JCO.2007.12.1087 URL |
| [22] |
SANDLUND J, OOSTERWIJK E, GRANKVIST K, et al. Prognostic impact of carbonic anhydrase Ⅸ expression in human renal cell carcinoma[J]. BJU Int, 2007, 100(3):556-560.
doi: 10.1111/bju.2007.100.issue-3 URL |
| [23] |
PATARD J J, FERGELOT P, KARAKIEWICZ P I, et al. Low CAIX expression and absence of VHL gene mutation are associated with tumor aggressiveness and poor survival of clear cell renal cell carcinoma[J]. Int J Cancer, 2008, 123(2):395-400.
doi: 10.1002/ijc.23496 URL |
| [24] |
SOYUPAK B, ERDOĞAN S, ERGIN M, et al. CA9 expression as a prognostic factor in renal clear cell carcinoma[J]. Urol Int, 2005, 74(1):68-73.
pmid: 15711113 |
| [25] |
LAGUNA M P. Re: carbonic anhydrase IX (CAIX) is not an independent predictor of outcome in patients with clear cell renal cell carcinoma (ccRCC) after long-term follow-up[J]. J Urol, 2014, 191(1):54-55.
doi: 10.1016/j.juro.2013.09.047 pmid: 24331469 |
| [26] |
ZERATI M, LEITE K R, PONTES-JUNIOR J, et al. Carbonic Anhydrase IX is not a predictor of outcomes in non-metastatic clear cell renal cell carcinoma-a digital analysis of tissue microarray[J]. Int Braz J Urol, 2013, 39(4):484-492.
doi: 10.1590/S1677-5538.IBJU.2013.04.05 URL |
| [1] | 王瀚, 陆海迪, 王雷, 丛文铭, 郑建明, 白辰光. 结肠鳞癌2例和腺鳞癌2例临床病理学特征分析[J]. 诊断学理论与实践, 2023, 22(01): 44-49. |
| [2] | 王瑾, 郭睿, 李彪, 张晓哲. 18F-FDG PET/CT显像动态评估自然杀伤/T细胞淋巴瘤(鼻型)治疗预后[J]. 诊断学理论与实践, 2022, 21(06): 702-709. |
| [3] | 谢吻, 梁怀予, 董磊, 袁菲, 王朝夫, 郭滟. 胰腺导管腺癌重要驱动基因突变与临床病理特征、预后间相关性的分析[J]. 诊断学理论与实践, 2022, 21(05): 581-587. |
| [4] | 李蕾, 袁菲, 王朝夫, 许海敏, 王婷. 101例壶腹部腺癌临床病理及预后因素分析[J]. 诊断学理论与实践, 2022, 21(03): 355-361. |
| [5] | 陈曦, 杜鹃. 多发性骨髓瘤预后风险的精准评估[J]. 诊断学理论与实践, 2021, 20(06): 522-528. |
| [6] | 冯国伟, 张晓娟, 郭睿, 关哲, 王越. 治疗前18F-FDG PET/CT显像对结外NK/T细胞淋巴瘤的预后判断价值[J]. 诊断学理论与实践, 2021, 20(06): 533-539. |
| [7] | 梁亚丽, 赵海港, 项广宇. 应激性高血糖比值预测急性缺血性脑卒中患者溶栓治疗后1年不良预后的价值[J]. 诊断学理论与实践, 2021, 20(06): 562-566. |
| [8] | 冯明洋, 丁叶舟, 赵青青, 赵钢德, 娄世珂, 郑超, 孙学华, 刘柯慧, 林兰意, 谢青, 郑岚, 王晖. 肝衰竭患者中医证型与西医肝衰竭分期之间的关系观察[J]. 诊断学理论与实践, 2021, 20(04): 391-395. |
| [9] | 芮文斌, 徐达, 祝宇, 吴瑜璇, 王浩飞, 汪成合, 袁菲. 缺氧诱导因子1α在乳头状肾细胞癌中的表达及其与预后的关系[J]. 诊断学理论与实践, 2021, 20(03): 265-370. |
| [10] | 刘彤, 王鑫. 心房颤动预后不良风险的评估策略[J]. 诊断学理论与实践, 2020, 19(06): 555-558. |
| [11] | 张中文, 左祥荣, 郑绪辉, 曹权, 李新立, 李艳秀. 3q26 rs12696304基因多态性与中国南方汉族老年人群急性心力衰竭患者一年预后间的关系研究[J]. 诊断学理论与实践, 2020, 19(06): 565-571. |
| [12] | 徐兆平, 王浩飞. ZNF692基因在肾透明细胞癌中的表达及其与患者预后间关系的研究[J]. 诊断学理论与实践, 2020, 19(03): 292-296. |
| [13] | 杜海磊, 陈聆, 罗方秀, 李勇, 程齐俭, 朱良纲, 杭钧彪. Beclin-1和Bcl-2表达与非小细胞肺癌患者病理特征及预后间关系的研究[J]. 诊断学理论与实践, 2020, 19(03): 258-263. |
| [14] | 杜云志, 冯菁华, 常春康. 二代测序技术在骨髓增生异常综合征临床诊断和治疗决策中的应用进展[J]. 诊断学理论与实践, 2019, 18(06): 685-671. |
| [15] | 张玉奇, 鲍圣芳. 血管环的产前超声心动图诊断及预后评估[J]. 诊断学理论与实践, 2019, 18(05): 487-490. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||