诊断学理论与实践 ›› 2021, Vol. 20 ›› Issue (06): 562-566.doi: 10.16150/j.1671-2870.2021.06.009
梁亚丽( ), 赵海港, 项广宇
), 赵海港, 项广宇
收稿日期:2021-04-15
出版日期:2021-12-25
发布日期:2021-12-25
通讯作者:
梁亚丽
E-mail:flydzf@163.com
LIANG Yali(), ZHAO Haigang, XIANG Guangyu
Received:2021-04-15
Online:2021-12-25
Published:2021-12-25
Contact:
LIANG Yali
E-mail:flydzf@163.com
摘要:
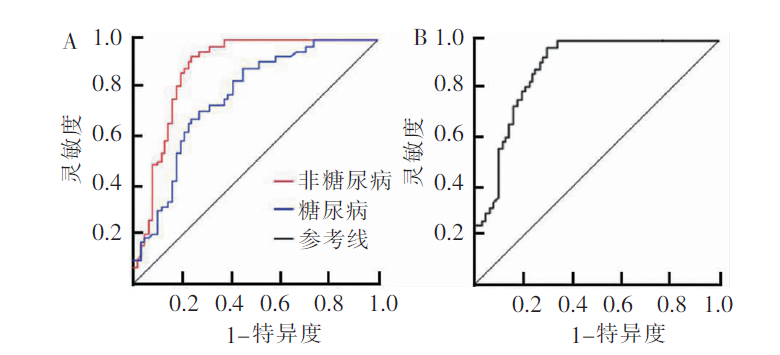
目的: 探讨应激性高血糖比值(stress hyperglycemia ratio,SHR)预测急性缺血性脑卒中患者出院后1年内出现不良预后的价值。方法: 收集2018年1月至2020年1月在我院接受溶栓治疗的急性缺血性脑卒中患者262例,其中糖尿病84例,非糖尿病178例。根据患者入院24 h内的平均SHR(非糖尿病组0.859,糖尿病组0.914),依据是否高于平均水平,将糖尿病及非糖尿病患者分别分为低SHR组和高SHR组。比较糖尿病及非糖尿病患者中低SHR组与高SHR组的一般临床资料和出院1年内的死亡率。用Cox单因素和多因素回归分析,观察患者出院后1年内预后不良的独立危险因素,用受试者操作特征(receiver operating curve,ROC)曲线评估SHR预测患者出院后1年内出现不良预后的临床价值。结果: 非糖尿病患者和糖尿病患者中高SHR组的NIHSS评分、应激性高血糖发病率、空腹血糖和糖化血红蛋白水平均高于低SHR组(P<0.05)。非糖尿病高SHR组出院后1年内的死亡率为32.9%(28/85),高于非糖尿病低SHR组17.2%(16/93), χ2=5.910,P=0.015;糖尿病高SHR组出院后1年内的死亡率为48.9%(22/45),高于糖尿病低SHR组(17.9%,7/39), χ2=8.848,P=0.003);且非糖尿病高SHR组出院后1年内的死亡率低于糖尿病高SHR组,差异有统计学意义( χ2=4.075,P=0.044)。多因素分析提示,NIHSS评分、应激性高血糖、糖化血红蛋白和SHR水平是影响所有急性缺血性脑卒中患者出院后1年预后的独立危险因素。SHR预测急性缺血性脑卒出院后1年不良结局的曲线下面积为0.841,95%CI为0.804~0.861,预测非糖尿病急性缺血性脑卒中患者的曲线下面积为0.897(95%CI为0.814~0.913)。结论: 高SHR影响急性缺血性脑卒中患者接受溶栓治疗出院后1年的存活率,是患者预后不良的独立危险因素。
中图分类号:
梁亚丽, 赵海港, 项广宇. 应激性高血糖比值预测急性缺血性脑卒中患者溶栓治疗后1年不良预后的价值[J]. 诊断学理论与实践, 2021, 20(06): 562-566.
LIANG Yali, ZHAO Haigang, XIANG Guangyu. The stress-induced hyperglycemia ratio in the prognosis prediction of patients with acute ischemic stroke one year after thrombolytic therapy[J]. Journal of Diagnostics Concepts & Practice, 2021, 20(06): 562-566.
表1
非糖尿病和糖尿病患者低SHR组与高SHR组一般资料比较[n(%)]
| 因素 | 非糖尿病组 | t/χ2 | P值 | 糖尿病组 | t/χ2值 | P值 | ||
|---|---|---|---|---|---|---|---|---|
| 低SHR组 | 高SHR组 | 低SHR组 | 高SHR组 | |||||
| 性别(男/女) | 54/39 | 52/33 | 0.179 | 0.673 | 25/14 | 26/19 | 0.350 | 0.554 |
| 年龄(岁) | 65.3±3.6 | 66.1±4.1 | 0.872 | 0.386 | 66.2±3.1 | 66.8±4.3 | 0.512 | 0.698 |
| 体指数(kg/m2) | 24.3±3.2 | 24.8±3.6 | 0.745 | 0.415 | 24.5±3.6 | 25.1±3.3 | 0.841 | 0.412 |
| 高血压病史 | 48(51.6) | 47(55.3) | 0.242 | 0.623 | 25(64.1) | 27(60.0) | 1.161 | 0.281 |
| 血脂异常 | 44(47.3) | 43(50.6) | 0.191 | 0.662 | 15(38.5) | 18(40.0) | 0.021 | 0.886 |
| 冠心病史 | 12(12.9) | 13(15.3) | 0.210 | 0.647 | 7(17.9) | 9(20.0) | 0.057 | 0.811 |
| 吸烟史 | 60(64.5) | 56(65.9) | 0.037 | 0.848 | 20(51.3) | 24(53.3) | 0.035 | 0.851 |
| NIHSS评分(分) | 10.6±2.5 | 14.6±3.1 | 5.025 | <0.001 | 12.3±3.2 | 16.3±3.6 | 5.362 | <0.001 |
| 应激性高血糖 | 4(4.3) | 27(31.8) | 23.289 | <0.001 | 10(25.6) | 32(71.1) | 17.297 | <0.001 |
| 空腹血糖(mmol/L) | 5.1±0.4 | 6.5±1.1 | 3.854 | 0.010 | 8.3±2.1 | 10.9±3.2 | 4.230 | 0.004 |
| HbA1c(%) | 4.6±0.5 | 5.1±0.3 | 3.562 | 0.026 | 8.1±1.5 | 9.5±1.7 | 3.421 | 0.030 |
| 甘油三酯(mmol/L) | 1.7±0.6 | 1.8±0.8 | 0.652 | 0.562 | 2.1±0.5 | 2.3±0.8 | 0.472 | 0.685 |
| 总胆固醇(mmol/L) | 4.2±0.8 | 4.4±0.8 | 1.256 | 0.108 | 4.4±0.9 | 4.5±1.0 | 0.068 | 0.914 |
| 高密度脂蛋白(mmol/L) | 1.0±0.3 | 1.1±0.3 | 0.582 | 0.625 | 0.9±0.3 | 1.0±0.2 | 0.652 | 0.514 |
| 低密度脂蛋白(mmol/L) | 2.8±0.7 | 2.6±0.7 | 1.325 | 0.085 | 2.5±0.8 | 2.6±0.8 | 0.952 | 0.301 |
表2
低SHR组与高SHR组间的出院后1年结局比较[n(%)]
| 结局 | 非糖尿病组 | 糖尿病组 | |||
|---|---|---|---|---|---|
| 低SHR组 | 高SHR组 | 低SHR组 | 高SHR组 | ||
| 死亡 | 16(17.2) | 28(32.9) | 7(17.9) | 23(51.1) | |
| 存活 | 77(82.8) | 57(67.1) | 32(82.1) | 22(48.9) | |
| χ2(P) | 5.910(0.015) | 8.848(0.003) | |||
表3
提示急性缺血性脑卒中患者出院后1年预后不良的危险因素
| 因素 | 单因素 | 多因素 | |||
|---|---|---|---|---|---|
| OR值(95%CI) | P值 | OR值(95%CI) | P值 | ||
| NIHSS评分 | 1.526(1.025~3.362) | 0.021 | 1.325(1.007~3.054) | 0.035 | |
| 应激性高血糖发生率 | 1.625(1.201~5.230) | 0.006 | 1.481(1.052~4.321) | 0.010 | |
| 空腹血糖 | 1.025(1.008~1.325) | 0.016 | 1.021(0.985~1.265) | 0.068 | |
| HbA1c | 1.652(1.214~4.326) | 0.004 | 1.526(1.158~3.415) | 0.016 | |
| SHR | 1.526(1.107~4.182) | 0.014 | 1.214(1.010~2.869) | 0.026 | |
图1
SHR对急性缺血性脑卒中出院后1年不良预后预测的ROC曲线 A:SHR预测糖尿病和非糖尿病急性缺血性脑卒中患者出院后1年预后不良;B:SHR预测急性缺血性脑卒中患者出院后1年预后不良。
| [1] |
Tziomalos K, Dimitriou P, Bouziana SD, et al. Stress hyperglycemia and acute ischemic stroke in-hospital outcome[J]. Metabolism, 2017, 67:99-105.
doi: 10.1016/j.metabol.2016.11.011 URL |
| [2] |
International Hypoglycaemia Study Group. Hypoglycaemia, cardiovascular disease, and mortality in diabetes: epidemiology, pathogenesis, and management[J]. Lancet Diabetes Endocrinol, 2019, 7(5):385-396.
doi: 10.1016/S2213-8587(18)30315-2 URL |
| [3] |
Roquer J, Giralt-Steinhauer E, Cerdà G, et al. Glycated hemoglobin value combined with initial glucose levels for evaluating mortality risk in patients with ischemic stroke[J]. Cerebrovasc Dis, 2015, 40(5-6):244-250.
doi: 10.1159/000440735 pmid: 26484656 |
| [4] |
Capes SE, Hunt D, Malmberg K, et al. Stress hyperglycaemia and increased risk of death after myocardial infarction in patients with and without diabetes: a systema-tic overview[J]. Lancet, 2000, 355(9206):773-778.
doi: 10.1016/S0140-6736(99)08415-9 pmid: 10711923 |
| [5] |
Roberts GW, Quinn SJ, Valentine N, et al. Relative Hyperglycemia, a marker of critical illness: introducing the stress hyperglycemia ratio[J]. J Clin Endocrinol Metab, 2015, 100(12):4490-4497.
doi: 10.1210/jc.2015-2660 URL |
| [6] |
Yang Y, Kim TH, Yoon KH, et al. The stress hyperglycemia ratio, an index of relative hyperglycemia, as a predictor of clinical outcomes after percutaneous coronary intervention[J]. Int J Cardiol, 2017, 241:57-63.
doi: 10.1016/j.ijcard.2017.02.065 URL |
| [7] | Liu N, Sheng J, Wang Y. Effect of stress hyperglycaemia on monocyte chemoattractant protein-1 levels and the short-term prognosis of patients with acute ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention[J]. Exp Ther Med, 2019, 17(5):3823-3829. |
| [8] |
Khopkar TP, Swami A. A study of stress hyperglycemia in acute myocardial infarction in non-diabetic patients[J]. J Assoc Physicians India, 2020, 68(1):54.
pmid: 31979594 |
| [9] | Scheen M, Giraud R, Bendjelid K. Stress hyperglycemia, cardiac glucotoxicity, and critically ill patient outcomes current clinical and pathophysiological evidence[J]. Physiol Rep, 2021, 9(2):e14713. |
| [10] | 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组. 中国急性缺血性脑卒中诊治指南2018[J]. 中华神经科杂志, 2018, 51(9):666-682. |
| [11] | Tanaka K, Tsutsumi YM. Glucose metabolism: stress hyperglycemia and glucose control[J]. Masui, 2016, 65(5):495-502. |
| [12] |
Ishihara M, Kojima S, Sakamoto T, et al. Acute hyperglycemia is associated with adverse outcome after acute myocardial infarction in the coronary intervention era[J]. Am Heart J, 2005, 150(4):814-820.
doi: 10.1016/j.ahj.2004.12.020 URL |
| [13] | 中国成人血脂异常防治指南修订联合委员会. 中国成人血脂异常防治指南(2016年修订版)[J]. 中国循环杂志, 2016, 31(10):937-950. |
| [14] |
Hamed SA. Brain injury with diabetes mellitus: evidence, mechanisms and treatment implications[J]. Expert Rev Clin Pharmacol, 2017, 10(4):409-428.
doi: 10.1080/17512433.2017.1293521 URL |
| [15] |
Kamada H, Yu F, Nito C, et al. Influence of hyperglycemia on oxidative stress and matrix metalloproteinase-9 activation after focal cerebral ischemia/reperfusion in rats: relation to blood-brain barrier dysfunction[J]. Stroke, 2007, 38(3):1044-1049.
doi: 10.1161/01.STR.0000258041.75739.cb URL |
| [16] |
Talukder RK, Uddin MJ, Battacharjee M, et al. Stress hyperglycemia and stroke outcome in patients with acute stroke[J]. Mymensingh Med J, 2018, 27(4):685-692.
pmid: 30487481 |
| [17] |
Yang Y, Kim TH, Yoon KH, et al. The stress hyperglycemia ratio, an index of relative hyperglycemia, as a predictor of clinical outcomes after percutaneous coronary intervention[J]. Int J Cardiol, 2017, 241:57-63.
doi: 10.1016/j.ijcard.2017.02.065 URL |
| [18] |
Kim YS, Kim C, Jung KH, et al. Range of glucose as a glycemic variability and 3-month outcome in diabetic patients with acute ischemic stroke[J]. PLoS One, 2017, 12(9):e0183894.
doi: 10.1371/journal.pone.0183894 URL |
| [19] | Marenzi G, Cosentino N, Milazzo V, et al. Prognostic va-lue of the acute-to-chronic glycemic ratio at admission in acute myocardial infarction: a prospective study[J]. Dia-betes Care, 2018, 41(4):847-853. |
| [20] |
Chu J, Tang J, Lai Y, et al. Association of stress hyperglycemia ratio with intracoronary thrombus burden in dia-betic patients with ST-segment elevation myocardial infarction[J]. J Thorac Dis, 2020, 12(11):6598-6608.
doi: 10.21037/jtd-20-2111 URL |
| [21] | 任燕霞. 应激性高血糖比值对急性心肌梗死患者院内预后的影响[D]. 大连医科大学, 2020. |
| [22] |
Kovacic JC, Castellano JM, Farkouh ME, et al. The relationships between cardiovascular disease and diabetes: focus on pathogenesis[J]. Endocrinol Metab Clin North Am, 2014, 43(1):41-57.
doi: 10.1016/j.ecl.2013.09.007 URL |
| [23] |
Mushtaq M, Abdul Mateen M, Kim UH. Hyperglycemia associated blood viscosity can be a nexus stimuli[J]. Clin Hemorheol Microcirc, 2019, 71(1):103-112.
doi: 10.3233/CH-180426 URL |
| [1] | 丁燕飞, 忻笑容, 周郁芬, 谢玲, 谷雷雷, 吴云林, 陈平. 上消化道溃疡伴出血患者溃疡愈合延迟的危险因素分析[J]. 诊断学理论与实践, 2022, 21(03): 312-316. |
| [2] | 刘安平, 凌枫, 史超, 孙璟. 上海社区老年脑卒中患者跌倒风险因素分析及风险识别模型的建立[J]. 诊断学理论与实践, 2021, 20(05): 475-479. |
| [3] | 施仲伟. 回眸过去30年全球和中国的心血管疾病负担及其危险因素——1990年至2019年全球心血管疾病负担及其危险因素报告解读[J]. 诊断学理论与实践, 2021, 20(04): 349-355. |
| [4] | 吴洁, 冯媛媛, 任妍, 曹久妹. 基于冠状动脉造影检查的高龄老年人群发生冠心病的危险因素调查及相应诊断模型的建立[J]. 诊断学理论与实践, 2021, 20(02): 201-206. |
| [5] | 林雨轩, 赵延华, 王筱婧. 丙泊酚镇静下无痛胃镜术中低氧血症的发生率及危险因素分析[J]. 诊断学理论与实践, 2020, 19(06): 594-599. |
| [6] | 魏晓敏, 张媛媛, 董樑, 夏敬文, 龚益, 喻永平, 李圣青. 真实世界中肺栓塞后慢性血栓栓塞性肺动脉高压的发病及相关危险因素前瞻性研究[J]. 诊断学理论与实践, 2019, 18(1): 37-43. |
| [7] | 周妍, 顾祎. 血清维生素D水平与老年人社区获得性肺炎严重程度的相关性研究[J]. 诊断学理论与实践, 2017, 16(06): 612-616. |
| [8] | 张诗, 何慧静, 万国斌. 200名晚期早产儿的盖塞尔婴幼儿智能评估量表的测试分析[J]. 诊断学理论与实践, 2017, 16(02): 217-220. |
| [9] | 周嘉, 罗悦玲, 李励, 冼晶, 梁杏欢, 黄振兴, 秦映芬, 罗佐杰,. 广西40岁以上人群代谢综合征及其危险因素调查[J]. 诊断学理论与实践, 2016, 15(04): 364-370. |
| [10] | 王芳, 章安迪,. 伴有多种危险因素的冠心病患者支架内再狭窄的影响因素[J]. 诊断学理论与实践, 2016, 15(03): 280-282. |
| [11] | 陈淳, 王家莉, 季承博, 布阿提卡木, 彭亦雩, 傅毅,. 抵抗素与脑梗死及其危险因素的相关性研究[J]. 诊断学理论与实践, 2015, 14(03): 279-282. |
| [12] | 余跃天, 朱琤, 毛恩强, 舒良, 殷荣, 李昱洁, 刘春艳, 曹建国, 皋源,. 阿托伐他汀对缺血性脑卒中患者医院获得性肺炎的影响[J]. 诊断学理论与实践, 2015, 14(02): 169-174. |
| [13] | 李畅, 董海蕴, 苏侃, 顾刚,. 心律植入装置感染相关危险因素分析[J]. 诊断学理论与实践, 2015, 14(02): 142-145. |
| [14] | 杜美玲, 杨新春, 蔡军,. 原发性高血压的危险因素和发病机制的新认识[J]. 诊断学理论与实践, 2012, 11(06): 554-557. |
| [15] | 魏素平, 张春和,. 胶质纤维酸性蛋白与急性缺血性脑卒中的相关性研究[J]. 诊断学理论与实践, 2012, 11(03): 306-307. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||