诊断学理论与实践 ›› 2022, Vol. 21 ›› Issue (03): 317-325.doi: 10.16150/j.1671-2870.2022.03.005
刘鹏, 严福华, 秦乐, 肖瑞杰( )
)
收稿日期:2022-01-05
出版日期:2022-06-25
发布日期:2022-08-17
通讯作者:
肖瑞杰
E-mail:xrj40702@rjh.com.cn
基金资助:
LIU Peng, YAN Fuhua, QIN Le, XIAO Ruijie()
Received:2022-01-05
Online:2022-06-25
Published:2022-08-17
Contact:
XIAO Ruijie
E-mail:xrj40702@rjh.com.cn
摘要:
目的:研究肥厚型心肌病(hypertrophic cardiomyopathy, HCM)患者左心室舒张功能的心脏磁共振(cardiac magnetic resonance, CMR)心肌应变率参数与心源性猝死风险间的关系。方法:纳入160例HCM患者和50名健康志愿者的CMR扫描数据,收集应变率(strain rate, SR)参数,包括左心室舒张期峰值径向应变率(radial strain rate, RSR)、圆周应变率(circumferential strain rate, CSR)和长轴应变率(longitudinal strain rate, LSR)。根据2014版欧洲心脏病学会(European Society of Cardiology, ESC)指南和2020版美国心脏病学会/美国心脏病协会(American College of Cardiology/American Heart Association, ACC/AHA)指南分别对患者进行心源性猝死(sudden cardiac death, SCD)风险分级,使用独立样本t检验比较同一指南定义下高风险与低风险2组间的舒张功能差异,用单因素方差分析比较2种指南定义下不同风险亚组间的舒张功能差异,对指南中的主要风险因素与舒张功能CMR应变率参数间的相关性进行线性回归分析。结果:HCM患者左心室舒张期SR绝对值较对照组显著降低(RSR,-1.27±0.60比-2.40±0.59;CSR,0.71±0.24比1.22±0.25;LSR,0.52±0.24比0.89±0.20,P均<0.05)。根据2014版ESC指南分层,SCD高风险患者(27例)的舒张期RSR绝对值较低风险患者显著降低(P<0.05),而两者间的CSR及LSR无差异;根据2020版ACC/AHA指南,SCD高风险患者(92例)舒张期的3个心肌SR指标绝对值均较低风险患者显著降低(P均<0.05)。对在2014 ESC中为低风险而在2020版ACC/AHA指南中为高风险的患者(65例),其舒张期SR绝对值与2种指南均为高风险的患者相仿,但显著低于2种指南中均为低风险的患者。在主要SCD危险因素中,舒张期心肌SR绝对值在左室壁最大厚度≥30 mm和延迟强化/左室心肌质量比值≥15%时绝对值显著降低,左室舒张功能受损严重,左室壁最大厚度、延迟强化/左室心肌质量比值与舒张期心肌SR均有显著相关性(相关系数r为RSR: 0.48/0.35, CSR: -0.42/-0.31, LSR: -0.37/-0.16, P均<0.05)。结论:CMR左心室心肌SR在SCD高风险患者中显著降低,且与部分危险因素具有相关性,可作为辅助评估SCD风险的潜在生物学标志物。
中图分类号:
刘鹏, 严福华, 秦乐, 肖瑞杰. 肥厚型心肌病左室舒张功能的心脏磁共振心肌应变率参数与猝死风险关系的研究[J]. 诊断学理论与实践, 2022, 21(03): 317-325.
LIU Peng, YAN Fuhua, QIN Le, XIAO Ruijie. Study on correlation of cardiac magnetic resonance strain rate parameters of left ventricular diastolic function with risk of sudden death in hypertrophic cardiomyopathy[J]. Journal of Diagnostics Concepts & Practice, 2022, 21(03): 317-325.
表1
2种指南的风险评估因素[9-10]
| 指南 | 风险评估因素 |
|---|---|
| 2014版ESC指南 | 5年风险率=1-0.998exp(预后指数) 其中,预后指数=[0.159 398 58 × 左室壁最大厚度(mm)] - [0.002 942 71 × 左室壁最大厚度2(mm2)] + [0.025 908 2 × 左房直径(mm)] + [0.004 461 31 × 最大静息下左室流出道压差(mmHg)] + [0.458 308 2 × 心源性猝死家族史] + [0.826 391 95 × 非持续性室性心动过速] + [0.716 503 61 × 无法解释的晕厥] - [0.017 999 34 × 临床评估年龄(岁)] |
| 2020版ACC/AHA指南 | ①心源性猝死家族史;②最大左室壁厚度≥30 mm;③无法解释的晕厥;④非持续性室性心动过速;⑤延迟强化/左室心肌质量≥15%;⑥终末期左室射血分数<50%;⑦左室心尖部室壁瘤 |
表2
HCM患者和对照组的基线特征[n(%)]
| 基线特征 | HCM患者 (n=160) | 对照组 (n=50) | P值 |
|---|---|---|---|
| 年龄(岁) | 53.96±15.21 | 52.45±11.01 | 0.561 |
| 性别 | 97(60.63) | 30(60.00) | 0.937 |
| 高血压 | 108(67.50) | 0(0) | <0.001 |
| 高脂血症 | 59(36.88) | 0(0) | <0.001 |
| 糖尿病 | 17(10.63) | 0(0) | <0.001 |
| 心源性猝死家族史 | 8(5.00) | 0(0) | <0.001 |
| 非持续性室性心动过速 | 5(3.13) | 0(0) | <0.001 |
| 无法解释的晕厥 | 21(13.13) | 0(0) | <0.001 |
| 二尖瓣反流 | 123(76.88) | 0(0) | <0.001 |
| 左心室舒张末期容积(mL) | 102.62±12.12 | 105.34±10.33 | 0.514 |
| 左心室收缩末期容积(mL) | 22.52±7.61 | 29.44±7.45 | <0.001 |
| 左心室射血分数(%) | 75.51±5.94 | 70.46±6.44 | <0.001 |
表3
HCM患者和对照组的舒张期心肌应变率比较
| 舒张期心肌应变率 | HCM组(n=160) | 对照组(n=50) | P值 |
|---|---|---|---|
| 径向峰值应变率(s-1) | -1.27±0.60 | -2.40±0.59 | <0.001 |
| 圆周峰值应变率(s-1) | 0.71±0.24 | 1.22±0.25 | <0.001 |
| 长轴峰值应变率(s-1) | 0.52±0.24 | 0.89±0.20 | <0.001 |
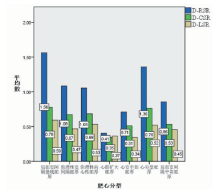
图1
不同分型HCM舒张期SR数据分布
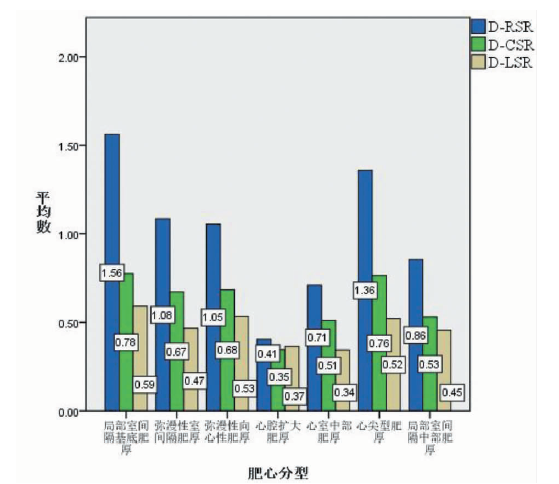
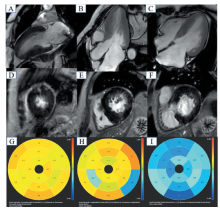
图2
2种指南低风险患者的电影序列(A~C)、延迟强化序列(D~F)和心肌应变率牛眼图(G~I) 注:患者,女,61岁,弥漫性室间隔肥厚,最大左室壁厚度为20 mm,延迟强化/左室心肌质量为9.64%,无心源性猝死家族史、非持续性室性心动过速和无法解释的晕厥。D-RSR、D-CSR和D-LSR分别为-1.28 s-1、0.7 s-1和0.34 s-1。根据2020版ACC/AHA指南和2014版ESC指南,该患者为心源性猝死低风险患者。
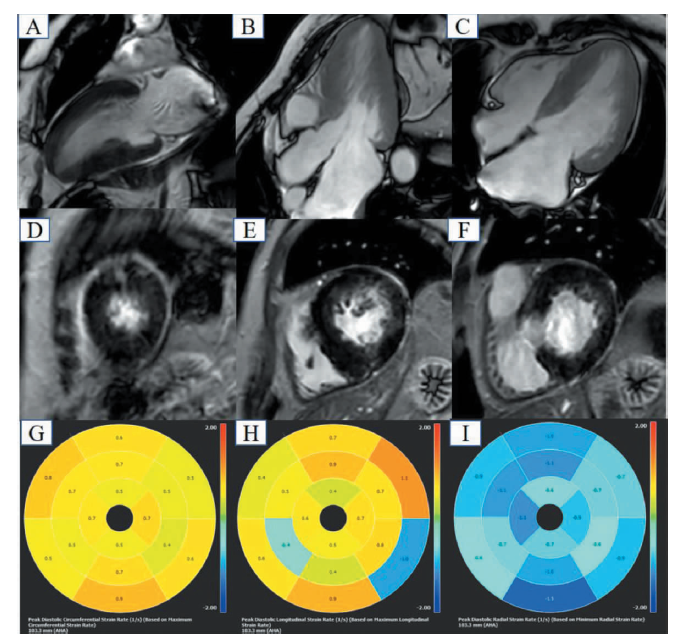
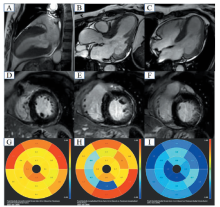
图3
2种指南风险不同患者的电影序列(A~C)、延迟强化序列(D~F)和心肌应变率牛眼图(G~I) 注:患者,女,53岁,局部室间隔基底肥厚,最大左室壁厚度为18 mm,延迟强化/左室心肌质量为13.91%,有心源性猝死家族史,无非持续性室性心动过速和无法解释的晕厥。D-RSR、D-CSR和D-LSR分别为-0.94 s-1、0.6 s-1和0.39 s-1。根据2014版ESC指南,该患者为心源性猝死低风险;根据2020版ACC/AHA指南,该患者为高风险。
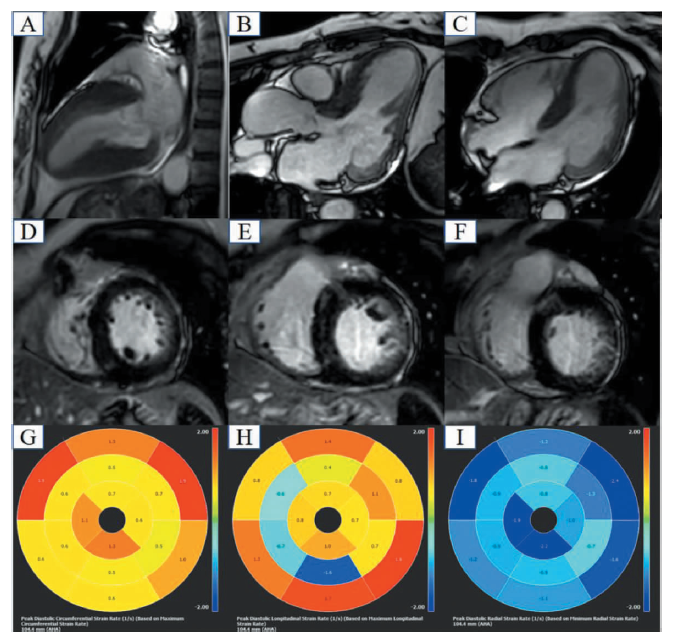
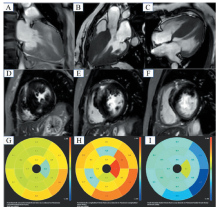
图4
2种指南高风险患者的电影序列(A~C)、延迟强化序列(D~F)和心肌应变率牛眼图(G~I) 注:患者,女,42岁,弥漫性室间隔肥厚,最大左室壁厚度为30 mm,延迟强化/左室心肌质量为31.28%,有心源性猝死家族史、无非持续性室性心动过速和无法解释的晕厥。D-RSR、D-CSR和D-LSR分别为-0.5 s-1、0.35 s-1和0.33 s-1。根据2020版ACC/AHA指南和2014版ESC指南,该患者为心源性猝死高风险。
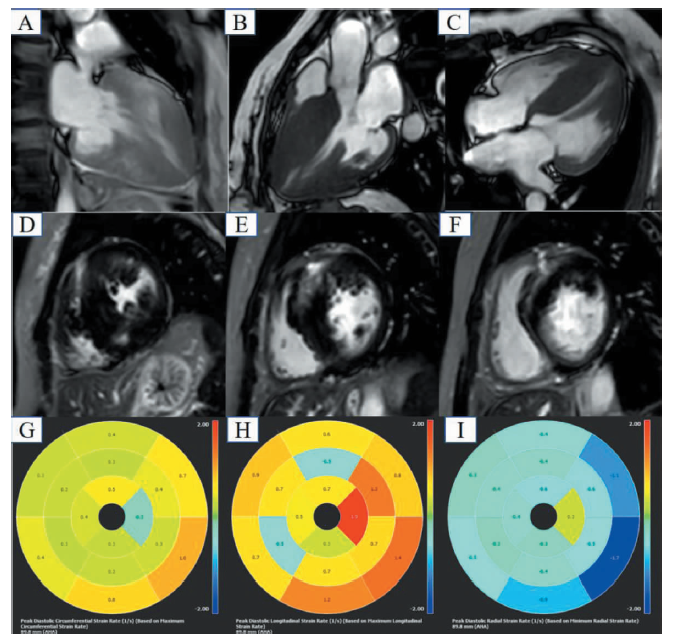
表4
2014 ESC指南中SCD不同风险患者的舒张期心肌应变率比较
| 舒张期心肌应变率 | 低风险 (n=133) | 高风险 (n=27) | t值 | P值 |
|---|---|---|---|---|
| 径向峰值应变率(s-1) | -1.31±0.62 | -1.06±0.48 | 1.99 | 0.048 |
| 圆周峰值应变率(s-1) | 0.72±0.24 | 0.65±0.25 | -1.29 | 0.201 |
| 长轴峰值应变率(s-1) | 0.52±0.23 | 0.54±0.29 | 0.40 | 0.691 |
表5
2020 ACC/AHA指南中SCD不同风险患者的舒张期心肌应变率比较
| 舒张期心肌应变率 | 低风险 (n=68) | 高风险 (n=92) | t值 | P值 |
|---|---|---|---|---|
| 径向峰值应变率(s-1) | -1.53±0.58 | -1.08±0.55 | 5.03 | <0.001 |
| 圆周峰值应变率(s-1) | 0.80±0.22 | 0.64±0.24 | -4.14 | <0.001 |
| 长轴峰值应变率(s-1) | 0.58±0.20 | 0.48±0.26 | -2.49 | 0.014 |
表6
不同风险等级HCM患者舒张期心肌应变率的比较
| 舒张期心肌应变率 | 亚组1 (n=68) | 亚组2 (n=65) | 亚组3 (n=27) | P值 |
|---|---|---|---|---|
| 径向峰值应变率(s-1) | -1.53±0.58 | -1.08±0.58 | -1.06±0.48 | <0.001 |
| 圆周峰值应变率(s-1) | 0.80±0.22 | 0.64±0.24 | 0.65±0.25 | <0.001 |
| 长轴峰值应变率(s-1) | 0.58±0.20 | 0.46±0.25 | 0.54±0.29 | 0.016 |
表7
HCM患者舒张期心肌应变率在不同危险因素分级中的比较
| 主要危险因素 | D-RSR(s-1) | t值 | P值 | D-CSR(s-1) | t值 | P值 | D-LSR(s-1) | t值 | P值 |
|---|---|---|---|---|---|---|---|---|---|
| MLVWT<30 mm(n=129) | -1.37±0.60 | 4.57 | <0.001 | 0.74±0.24 | -3.74 | <0.001 | 0.55±0.21 | -3.17 | <0.001 |
| MLVWT≥30 mm(n=31) | -0.85±0.41 | 0.57±0.21 | 0.40±0.33 | ||||||
| 左房直径<40 mm(n=27) | -1.41±0.69 | 1.38 | 0.169 | 0.77±0.28 | -1.58 | 0.117 | 0.52±0.27 | 0.04 | 0.965 |
| 左房直径≥40 mm(n=133) | -1.24±0.58 | 0.69±0.23 | 0.52±0.24 | ||||||
| 左室流出道压差<30 mmHG(n=56) | -1.14±0.60 | -1.99 | 0.048 | 0.68±0.27 | 1.17 | 0.244 | 0.51±0.22 | 0.60 | 0.548 |
| 左室流出道压差≥30 mmHG(n=104) | -1.34±0.60 | 0.72±0.23 | 0.53±0.25 | ||||||
| LGE/LVM比值<15%(n=87) | -1.46±0.63 | 4.63 | <0.001 | 0.77±0.24 | -3.56 | <0.001 | 0.55±0.24 | -1.77 | 0.024 |
| LGE/LVM比值≥15%(n=73) | -1.04±0.49 | 0.64±0.22 | 0.49±0.24 |
表8
回归分析HCM患者舒张期心肌应变率和不同危险因素的关系
| 指标 | MLVWT | 左房直径 | 左室流出道压差 | LGE/LVM比值 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| β | P值 | β | P值 | β | P值 | β | P值 | ||||
| D-RSR | 0.48 | <0.001 | 0.29 | <0.001 | -0.07 | 0.388 | 0.35 | <0.001 | |||
| D-CSR | -0.42 | <0.001 | -0.29 | <0.001 | 0.03 | 0.722 | -0.31 | <0.001 | |||
| D-LSR | -0.37 | <0.001 | -0.13 | 0.108 | -0.04 | 0.614 | -0.16 | 0.046 | |||
| [1] | 中国医师协会心力衰竭专业委员会, 中华心力衰竭和心肌病杂志编辑委员会. 中国肥厚型心肌病管理指南2017[J]. 中华心力衰竭和心肌病杂志(中英文), 2017, 1(2):65-86. |
| Heart Failure Professional Commi of Chinese Medical Docter Association, Eolitorial Board of Chinese Journal of Heart Failure and Cardiomyopathy. Eolitorial Board of Chinese Journal of Heart Failure and Cardiomyopathy. Chinese guildelines on the management of hypertrophic cardimyopathy 2017[J]. Chin J Heart Fail & Cardiomyopathy, 2017, 1(2):65-86. | |
| [2] | 雷晓琳, 陈石(综述), 陈玉成(审校). 心脏磁共振成像新技术及其在肥厚型心肌病研究中的应用[J]. 心血管病学进展, 2015(4):483-487. |
| Lei XL, Chen S, Chen YC. Cardiac magnetic resonance new technologies and its application for investigation in hypertrophic cardiomyopathy[J]. Advances in Cardiovascular Diseases, 2015, 36(4):483-487. | |
| [3] |
Scatteia A, Baritussio A, Bucciarelli-Ducci C. Strain imaging using cardiac magnetic resonance[J]. Heart Fail Rev, 2017, 22(4):465-476.
doi: 10.1007/s10741-017-9621-8 pmid: 28620745 |
| [4] | 李亚萍, 赵蕾, 范占明. MR应变成像技术在心脏疾病中的应用[J]. 中国医学影像技术, 2018, 34(4):621-624. |
| Li YP, Zhao L, Fan ZM. Application of MR strain ima-ging in cardiac diseases[J]. Chinese Journal of Medical Imaging Technology, 2018, 34(4):621-624. | |
| [5] |
Swoboda PP, McDiarmid AK, Erhayiem B, et al. Effect of cellular and extracellular pathology assessed by T1 mapping on regional contractile function in hypertrophic cardiomyopathy[J]. J Cardiovasc Magn Reson, 2017, 19(1):16.
doi: 10.1186/s12968-017-0334-x URL |
| [6] | 徐刚. 心脏磁共振在肥厚型心肌病中的临床应用研究[D]. 第三军医大学, 2015. |
| Xu G. Clinical application study of cardiac magnetic reso-nance on hypertrophic cardiomyopathy[D]. Army Medical University, 2015. | |
| [7] |
Chen S, Yuan J, Qiao S, et al. Evaluation of left ventri-cular diastolic function by global strain rate imaging in patients with obstructive hypertrophic cardiomyopathy: a simultaneous speckle tracking echocardiography and cardiac catheterization study[J]. Echocardiography, 2014, 31(5):615-622.
doi: 10.1111/echo.12424 pmid: 24219240 |
| [8] |
Baxi AJ, Restrepo CS, Vargas D, et al. Hypertrophic cardiomyopathy from A to Z: cenetics, pathophysiology, imaging, and management[J]. Radiographics, 2016, 36(2):335-354.
doi: 10.1148/rg.2016150137 URL |
| [9] |
Authors/Task Force members, Elliott PM, Anastasakis A, et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: the task force for the diagnosis and management of hypertrophic cardiomyopathy of the European Society of Cardiology(ESC)[J]. Eur Heart J, 2014, 35(39):2733-2779.
doi: 10.1093/eurheartj/ehu284 pmid: 25173338 |
| [10] | Ommen SR, Mital S, Burke MA, et al. 2020 AHA/ACC Guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines[J]. CJ Am Coll Cardiol, 2020, 76(25):e159-e240. |
| [11] |
Smiseth OA, Torp H, Opdahl A, et al. Myocardial strain imaging: how useful is it in clinical decision making?[J]. Eur Heart J, 2016, 37(15):1196-1207.
doi: 10.1093/eurheartj/ehv529 pmid: 26508168 |
| [12] |
Zhu L, Gu S, Wang Q, et al. Left ventricular myocardial deformation: a study on diastolic function in the Chinese male population and its relationship with fat distribution[J]. Quant Imaging Med Surg, 2020, 10(3):634-645.
doi: 10.21037/qims.2020.01.16 URL |
| [13] | Kermer J, Traber J, Utz W, et al. Assessment of diastolic dysfunction: comparison of different cardiovascular magnetic resonance techniques[J]. ESC Heart Fail, 2020, 7(5):2637-2649. |
| [14] | Kuo JY, Chang SH, Sung KT, et al. Left ventricular dysfunction in atrial fibrillation and heart failure risk[J]. ESC Heart Fail, 2020, 7(6):3694-3706. |
| [15] |
Maron MS, Rowin EJ, Wessler BS, et al. Enhanced American College of Cardiology/American Heart Association Strategy for prevention of sudden cardiac death in high-risk patients with hypertrophic cardiomyopathy[J]. JAMA Cardiol, 2019, 4(7):644-657.
doi: 10.1001/jamacardio.2019.1391 URL |
| [16] |
Lin TT, Wang YC, Juang JJ, et al. Application of the newest European Association of Cardiovascular Imaging Recommendation regarding the long-term prognostic relevance of left ventricular diastolic function in heart failure with preserved ejection fraction[J]. Eur Radiol, 2020, 30(1):630-639.
doi: 10.1007/s00330-019-06261-1 URL |
| [17] |
Yokoi T, Morimoto R, Oishi H, et al. Left ventricular relaxation half-time as a predictor of cardiac events in idiopathic dilated cardiomyopathy and hypertrophic cardiomyopathy with Left ventricular systolic and/or diastolic dysfunction[J]. Am J Cardiol, 2019, 124(3):435-441.
doi: 10.1016/j.amjcard.2019.05.005 URL |
| [18] |
Villemain O, Correia M, Mousseaux E, et al. Myocardial stiffness evaluation using noninvasive shear wave imaging in healthy and hypertrophic cardiomyopathic adults[J]. JACC Cardiovasc Imaging, 2019, 12(7 Pt 1):1135-1145.
doi: S1936-878X(18)30140-2 pmid: 29550319 |
| [19] |
Chacko BR, Karur GR, Connelly KA, et al. Left ventricular structure and diastolic function by cardiac magnetic resonance imaging in hypertrophic cardiomyopathy[J]. Indian Heart J, 2018, 70(1):75-81.
doi: 10.1016/j.ihj.2016.12.021 URL |
| [20] |
Yang H, Carasso S, Woo A, et al. Hypertrophy pattern and regional myocardial mechanics are related in septal and apical hypertrophic cardiomyopathy[J]. J Am Soc Echocardiogr, 2010, 23(10):1081-1089.
doi: 10.1016/j.echo.2010.06.006 URL |
| [21] |
Kim EK, Lee SC, Hwang JW, et al. Differences in apical and non-apical types of hypertrophic cardiomyopathy: a prospective analysis of clinical, echocardiographic, and cardiac magnetic resonance findings and outcome from 350 patients[J]. Eur Heart J Cardiovasc Imaging, 2016, 17(6):678-686.
doi: 10.1093/ehjci/jev192 URL |
| [22] |
Villa AD, Sammut E, Zarinabad N, et al. Microvascular ischemia in hypertrophic cardiomyopathy: new insights from high-resolution combined quantification of perfusion and late gadolinium enhancement[J]. J Cardiovasc Magn Reson, 2016, 18:4.
doi: 10.1186/s12968-016-0223-8 URL |
| [23] |
Ellims AH, Iles LM, Ling LH, et al. Diffuse myocardial fibrosis in hypertrophic cardiomyopathy can be identified by cardiovascular magnetic resonance, and is associated with left ventricular diastolic dysfunction[J]. J Cardiovasc Magn Reson, 2012, 14(1):76.
doi: 10.1186/1532-429X-14-76 URL |
| [24] |
Kanagala P, Cheng ASH, Singh A, et al. Relationship between focal and diffuse fibrosis assessed by CMR and clinical outcomes in heart failure with preserved ejection graction[J]. JACC Cardiovasc Imaging, 2019, 12(11 Pt 2):2291-2301.
doi: S1936-878X(19)30075-0 pmid: 30772227 |
| [25] |
Avegliano G, Politi MT, Costabel JP, et al. Differences in the extent of fibrosis in obstructive and nonobstructive hypertrophic cardiomyopathy[J]. J Cardiovasc Med (Hagerstown), 2019, 20(6):389-396.
doi: 10.2459/JCM.0000000000000800 URL |
| [26] |
Satriano A, Heydari B, Guron N, et al. 3-Dimensional regional and global strain abnormalities in hypertrophic cardiomyopathy[J]. Int J Cardiovasc Imaging, 2019, 35(10):1913-1924.
doi: 10.1007/s10554-019-01631-8 URL |
| [1] | 黄少华, 梁宗辉, 童欢, 管雪妮, 郭瑛, 张雁, 曹宾, 孙育民. 心脏磁共振评估强直性肌营养不良1型患者心肌纤维化的临床价值[J]. 诊断学理论与实践, 2021, 20(04): 362-367. |
| [2] | 朱兰, 顾圣佳, 陈炽华, 曹琪琪, 周皛月, 严福华, 闵佶华. 基于可变形配准算法的心肌形变分析对肥厚型心肌病的诊断及预后预测的价值探讨[J]. 诊断学理论与实践, 2019, 18(03): 278-285. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||