诊断学理论与实践 ›› 2022, Vol. 21 ›› Issue (03): 349-354.doi: 10.16150/j.1671-2870.2022.03.010
刘萍a, 肖园a, 王歆琼a, 陆亭伟b, 赵雪松c, 杨媛艳a( )
)
收稿日期:2022-01-14
出版日期:2022-06-25
发布日期:2022-08-17
通讯作者:
杨媛艳
E-mail:yyy21471@126.com
LIU Pinga, XIAO Yuana, WANG Xinqionga, LU Tingweib, ZHAO Xuesongc, YANG Yuanyana()
Received:2022-01-14
Online:2022-06-25
Published:2022-08-17
Contact:
YANG Yuanyan
E-mail:yyy21471@126.com
摘要:
目的:分析1例克罗恩病合并Wiskott-Aldrich综合征(Wiskott-Aldrich syndrome, WAS)患儿的临床、结肠镜表现及其基因特征,为临床诊断提供参考。方法:回顾性分析1例克罗恩病合并WAS患儿的临床表现和生化指标、结肠镜检查、基因检测结果以及其治疗、随访情况,并在PubMed、中国知网、万方数据库中检索相关文献,综合分析。结果:患儿为6岁男童,表现为反复腹痛、便血1个月及肛周脓肿半个月,并从婴儿期出现血小板计数减少。实验室检查提示患儿存在中度贫血(血红蛋白70 g/L),血小板(77×109/L)降低,红细胞沉降率(71 mm/h)升高,粪钙卫蛋白(大于1 800 μg/g)升高;电子结肠镜检查提示结肠多发溃疡,肠镜活检病理提示末端回肠及全结肠黏膜慢性活动性炎,部分伴局灶微脓肿和隐窝脓肿。该患儿被诊断为克罗恩病。基因检测显示其WAS基因外显子8上剪接位点出现半合子突变(c.777+3_777+6del GAGT),根据美国医学遗传与基因组学学会指南,该突变为可能致病性突变,故确诊为克罗恩病合并WAS。文献复习共检索到9篇炎症性肠病(inflammatory bowel disease, IBD)合并WAS基因突变病例的文献,共16例患者,均为幼年起病(1 d~14.9岁),其中10例伴有血小板减少。治疗方法包括药物、手术及骨髓移植等,获得随访的7例患者中有3例死亡。结论:对于儿童IBD患者,尤其是极早发型儿童IBD患者,应考虑单基因突变致病的可能性,如男性IBD患儿伴有自幼出现的血小板减少时,应检测WAS基因。
中图分类号:
刘萍, 肖园, 王歆琼, 陆亭伟, 赵雪松, 杨媛艳. Wiskott-Aldrich综合征合并克罗恩病一例并文献复习[J]. 诊断学理论与实践, 2022, 21(03): 349-354.
LIU Ping, XIAO Yuan, WANG Xinqiong, LU Tingwei, ZHAO Xuesong, YANG Yuanyan. Crohn′s disease in a child with Wiskott-Aldrich syndrome: a case report and literature review[J]. Journal of Diagnostics Concepts & Practice, 2022, 21(03): 349-354.
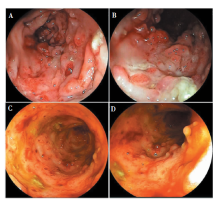
图1
电子肠镜检查 A、B:入我院时电子肠镜检查,见肠黏膜散在溃疡,表面附着白苔,周边黏膜水肿增生,部分呈指状隆起;C、D:随访电子肠镜检查,见肠黏膜糜烂,部分肠段见大片深溃疡,上覆脓苔,见较多炎性息肉样隆起。
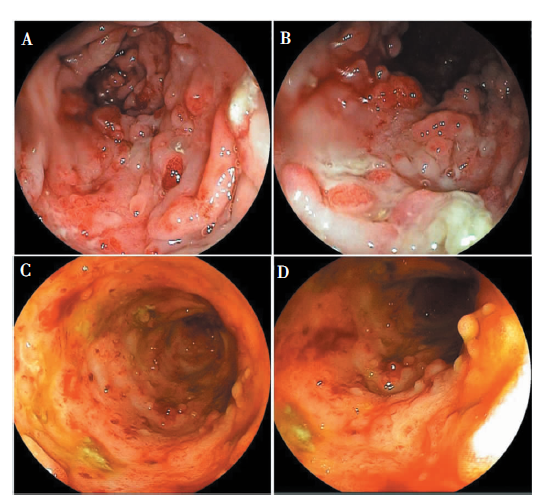
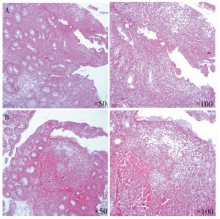
图2
患儿结肠黏膜病理图片 注:见慢性炎伴活动性炎,伴局灶糜烂,回盲部局灶微脓肿,可见个别隐窝脓肿。A:回盲部;B:降结肠。
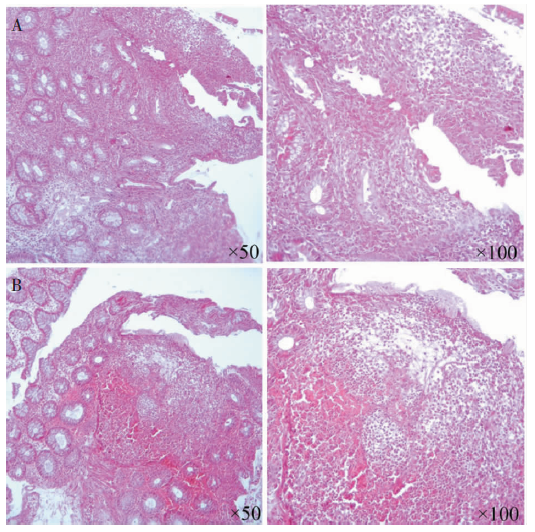
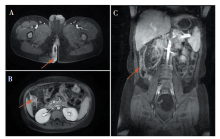
图3
盆腔及小肠MRI图片 A:盆腔增强MRI扫描,箭头所示提示肛瘘、肛周脓肿;B、C:小肠增强MRI扫描,箭头所示见右半结肠肠壁增厚,黏膜息肉样增生改变。
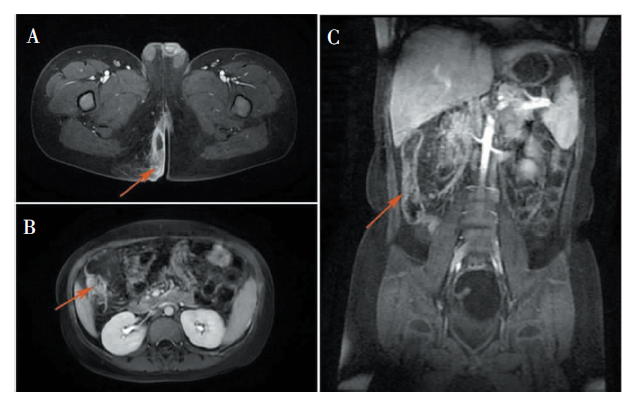

图4
患儿及其母亲基因测序结果 注:箭头所示为突变位点。A:患儿WAS基因外显子8检测到缺失变异c.777+3_777+6delGAGT(半合);B:患儿母亲WAS基因外显子8检测到缺失变异c.777+3_777+6delGAGT(杂合)。
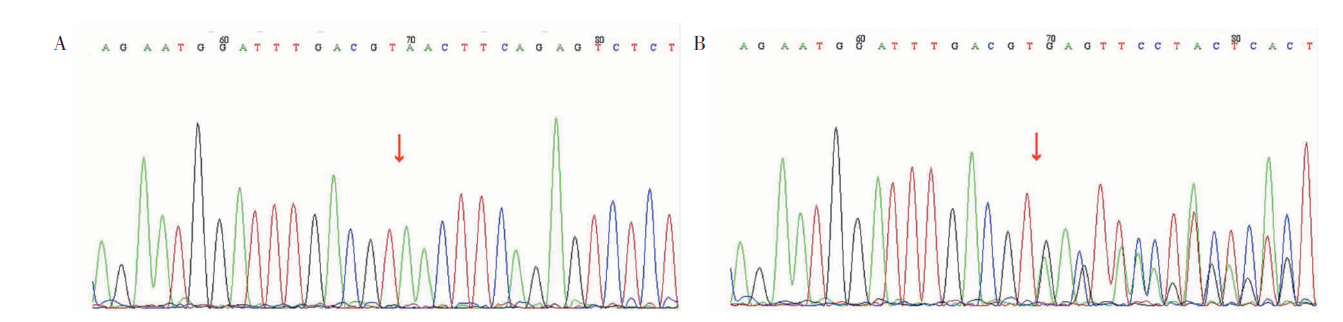
表1
文献复习资料
| 文献出处 | 发病年龄 | 肠道表现 | WAS相关表现 | 其他表现 | 基因突变 | 治疗 | 预后 |
|---|---|---|---|---|---|---|---|
| Folwaczny[ | 幼时 | UC | 血小板低,反复感染 | 无 | c.95C>T | 泼尼松龙、美沙拉嗪, 结肠切除术 | 死亡 |
| Cannioto[ | 15 d | CD | 血小板低,湿疹 | 无 | - | 骨髓移植 | 缓解 |
| 1 d | IBD-U | 血小板低,湿疹 | 无 | - | 骨髓移植 | 死亡(18个月) | |
| 1 d | UC | 血小板低 | 无 | - | 骨髓移植 | 死亡(16个月) | |
| Ohya[ | 12岁 | CD | 湿疹 | 无 | c.1378C>T,p.P460S | 美沙拉嗪、硫唑嘌呤、 英夫利昔单抗 | 缓解 |
| 11岁 | UC | 无 | 无 | c.1378C>T,p.P460S | 美沙拉嗪、硫唑嘌呤 | 缓解 | |
| 2岁 | UC | 无 | 无 | c.1378C>T,p.P460S | 美沙拉嗪、泼尼松龙灌肠 | 缓解 | |
| Ashton[ | 11.5岁 | UC | 间歇性血小板减少、 反复感染 | 原发性硬化 性胆管炎 | c.1378C>T,p.P460S | 硫唑嘌呤、英夫利昔单抗、 阿达木、全结肠切除 | - |
| 14.9岁 | UC | 无 | 原发性硬 化性胆管炎 | c.1378C>T,p.P460S | 硫唑嘌呤、全结肠切除 | - | |
| 14.3岁 | CD | 无 | 肛周脓肿、 肛瘘 | c.391G>A,p.E131K | 硫唑嘌呤,肛周手术 | - | |
| 13.5岁 | CD | 无 | 无 | c.391G>A,p.E131K | 硫唑嘌呤、英夫利昔单抗 | - | |
| Esmaeilzadeh[ | 8个月 | UC | 血小板低,反复感染 | 无 | c.360+1G>C | - | - |
| Zhang[ | 20 d | IBD | 血小板低、湿疹 | 无 | 431G>A | - | - |
| 23 d | IBD | 血小板低、湿疹 | 无 | IVS8+1 to +6delGAGT | - | - | |
| 2个月 | IBD | 血小板低、湿疹 | 无 | 923-924 dupGC | - | - | |
| 3个月 | IBD | 血小板低、湿疹 | 无 | IVS8+1 G>A | - | - |
| [1] |
Loftus EV Jr. Clinical epidemiology of inflammatory bowel disease: Incidence, prevalence, and environmental in-fluences[J]. Gastroenterology, 2004, 126(6):1504-1517.
doi: 10.1053/j.gastro.2004.01.063 URL |
| [2] |
Heyman MB, Kirschner BS, Gold BD, et al. Children with early-onset inflammatory bowel disease (IBD): analysis of a pediatric IBD consortium registry[J]. J Pediatr, 2005, 146(1):35-40.
doi: 10.1016/j.jpeds.2004.08.043 URL |
| [3] | Nameirakpam J, Rikhi R, Rawat SS, et al. Genetics on early onset inflammatory bowel disease: an update[J]. Genes Dis, 2019, 7(1):93-106. |
| [4] |
Uhlig HH. Monogenic diseases associated with intestinal inflammation: implications for the understanding of inflammatory bowel disease[J]. Gut, 2013, 62(12):1795-1805.
doi: 10.1136/gutjnl-2012-303956 pmid: 24203055 |
| [5] | 中华医学会儿科学分会消化学组, 中华医学会儿科学分会临床营养学组. 儿童炎症性肠病诊断和治疗专家共识[J]. 中华儿科杂志, 2019, 57(7):501-507. |
| The Subspecialty Group of Gastroenterology, the Society of Pediatrics, Chinese Medical Association, the Subspecialty Group of Clinical Nutrition, the Society of Pedia-trics, Chinese Medical Association. Chinese Medical Association. Expert consensus on the diagnosis and management of pediatric inflammatory bowel disease[J]. Chin J Pediatr, 2019, 57(7):501-507. | |
| [6] |
Richards S, Aziz N, Bale S, et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology[J]. Genet Med, 2015, 17(5):405-424.
doi: 10.1038/gim.2015.30 pmid: 25741868 |
| [7] |
Folwaczny C, Ruelfs C, Walther J, et al. Ulcerative colitis in a patient with Wiskott-Aldrich syndrome[J]. Endoscopy, 2002, 34(10):840-841.
pmid: 12244510 |
| [8] |
Cannioto Z, Berti I, Martelossi S, et al. IBD and IBD mimicking enterocolitis in children younger than 2 years of age[J]. Eur J Pediatr, 2009, 168(2):149-155.
doi: 10.1007/s00431-008-0721-2 pmid: 18546019 |
| [9] |
Ohya T, Yanagimachi M, Iwasawa K, et al. Childhood-onset inflammatory bowel diseases associated with mutation of Wiskott-Aldrich syndrome protein gene[J]. World J Gastroenterol, 2017, 23(48):8544-8552.
doi: 10.3748/wjg.v23.i48.8544 URL |
| [10] |
Ashton JJ, Mossotto E, Stafford IS, et al. Genetic sequencing of pediatric patients identifies mutations in monogenic inflammatory bowel disease genes that translate to distinct clinical phenotypes[J]. Clin Transl Gastroenterol, 2020, 11(2):e00129.
doi: 10.14309/ctg.0000000000000129 URL |
| [11] |
Esmaeilzadeh H, Bordbar MR, Dastsooz H, et al. A novel splice site mutation in WAS gene in patient with Wiskott-Aldrich syndrome and chronic colitis: a case report[J]. BMC Med Genet, 2018, 19(1):123.
doi: 10.1186/s12881-018-0647-0 pmid: 30029636 |
| [12] | Zhang L, Li YY, Tang X, et al. Faecal microbial dysbiosis in children with Wiskott-Aldrich syndrome[J]. Scand J Immunol, 2020, 91(1):e12805. |
| [13] |
Uhlig HH, Schwerd T, Koletzko S, et al. The diagnostic approach to monogenic very early onset inflammatory bowel disease[J]. Gastroenterology, 2014, 147(5):990-1007.
doi: 10.1053/j.gastro.2014.07.023 pmid: 25058236 |
| [14] | Öztürk ZA, Dag MS, Kuyumcu ME, et al. Could platelet indices be new biomarkers for inflammatory bowel di-seases?[J]. Eur Rev Med Pharmacol Sci, 2013, 17(3):334-341. |
| [15] |
Candotti F. Clinical Manifestations and Pathophysiological Mechanisms of the Wiskott-Aldrich Syndrome[J]. J Clin Immunol, 2018, 38(1):13-27.
doi: 10.1007/s10875-017-0453-z pmid: 29086100 |
| [16] | Dupuis-Girod S, Medioni J, Haddad E, et al. Autoimmunity in Wiskott-Aldrich syndrome: risk factors, clinical features, and outcome in a single-center cohort of 55 patients[J]. Pediatrics, 2003, 111(5 Pt 1):e622-e627. |
| [17] |
Brooimans RA, van den Berg AJ, Tamminga RY, et al. Identification of six novel WASP gene mutations in patients suffering from Wiskott-Aldrich syndrome[J]. Hum Mutat, 2000, 15(4):386-387.
doi: 10.1002/(SICI)1098-1004(200004)15:4<386::AID-HUMU23>3.0.CO;2-4 pmid: 10737997 |
| [1] | 吴霜, 解骞, 管雪妮, 张素芳, 高信芳, 梁宗辉. 磁共振体素内不相干运动扩散加权成像诊断活动期克罗恩病的价值及效能分析[J]. 诊断学理论与实践, 2020, 19(02): 157-161. |
| [2] | 叶成林, 姚永华, 陈真, 贾麟. 骨髓活检塑胶包埋在以单纯血小板减少为表现的骨髓增生异常综合征诊断中的应用价值[J]. 诊断学理论与实践, 2020, 19(02): 177-181. |
| [3] | 刘晓依, 陈琢, 吴静, 金莹莹, 陈同辛, 陈戟. 四种常见原发性免疫缺陷病的临床感染和皮肤表现[J]. 诊断学理论与实践, 2019, 18(04): 442-447. |
| [4] | 余悠悠, 曾俊祥, 罗婷, 邓琳, 潘秀军. 三种不同品牌ELISA试剂盒检测ASCA的结果比较及性能评估[J]. 诊断学理论与实践, 2019, 18(04): 454-459. |
| [5] | 常蕊, 徐嘉旭, 董海鹏, 吴梦雄, 赵雪松, 缪飞, 严福华. CT能谱成像在小肠克恩罗恩病活动度评估中的价值[J]. 诊断学理论与实践, 2019, 18(04): 432-435. |
| [6] | 杨媛艳, 肖园, 陈晓炎, 苏雯, 许春娣, 张清清. PIK3CDδ过度活化综合征一例并文献复习[J]. 诊断学理论与实践, 2019, 18(03): 296-300. |
| [7] | 曾俊祥, 罗婷, 葛文松, 潘秀军, 沈立松. 抗GP2和抗CUZD1抗体对克罗恩病的诊断价值评估[J]. 诊断学理论与实践, 2018, 17(04): 433-438. |
| [8] | 李坦, 李斌, 刘媛媛, 鲍扬漪. 原发免疫性血小板减少症患者外周血Treg细胞程序性死亡受体-1的表达[J]. 诊断学理论与实践, 2018, 17(03): 294-298. |
| [9] | 王敏敏, 曾惠, 郭晓珺. CD4+CD25+CD127-/low调节性T细胞和Th17细胞在ITP发病中的研究进展[J]. 诊断学理论与实践, 2018, 17(02): 220-224. |
| [10] | 蔡晓红, 雷航, 王学锋. 2017年英国血液学标准委员会《血小板输注指南》和要点解读[J]. 诊断学理论与实践, 2017, 16(03): 264-269. |
| [11] | 杨丽艳, 王化泉. 血小板生成素受体激动剂的作用机制及其在骨髓增生异常综合征治疗中的应用[J]. 诊断学理论与实践, 2016, 15(06): 567-572. |
| [12] | 韩晓凤, 倪蓓文, 方怡, 殷婷玉, 陈云燕, 朱照辉, 陈芳源,. 妊娠合并原发免疫性血小板减少症患者的临床特点分析及T细胞分泌细胞因子水平的研究[J]. 诊断学理论与实践, 2016, 15(02): 152-156. |
| [13] | 席瑜玲, 梁宗辉, 叶涛,. 克罗恩病的影像学诊断的研究进展[J]. 诊断学理论与实践, 2016, 15(01): 57-60. |
| [14] | 邱进锋, 王端旭, 张森, 张摇威, 纪少娜, 易海宁, 赵佳强, 尹俊,. 成人慢性免疫性血小板减少性紫癜患者血小板G蛋白偶联受体的研究[J]. 诊断学理论与实践, 2015, 14(06): 539-544. |
| [15] | 张悦民, 王剑飚, 陈骊婷,. 阿米卡星在1例多抗凝剂依赖性假性血小板减少症中的应用研究[J]. 诊断学理论与实践, 2015, 14(05): 437-440. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||