内科理论与实践 ›› 2022, Vol. 17 ›› Issue (05): 373-378.doi: 10.16138/j.1673-6087.2022.05.005
刘锐锋, 盛倩倩, 张悦, 赵慧强( )
)
收稿日期:2021-10-08
出版日期:2022-09-30
发布日期:2022-11-04
通讯作者:
赵慧强
E-mail:zhaohq05@aliyun.com
基金资助:
LIU Ruifeng, SHENG Qianqian, ZHANG Yue, ZHAO Huiqiang()
Received:2021-10-08
Online:2022-09-30
Published:2022-11-04
Contact:
ZHAO Huiqiang
E-mail:zhaohq05@aliyun.com
摘要:
目的:初步确定外周淋巴细胞和单核细胞是否参与了冠状动脉(冠脉)扩张(coronary artery ectasia, CAE)的病理过程,以推测CAE是否为免疫性疾病。方法:纳入2017年1月至2018年1月接受冠脉造影并确诊的34例CAE患者,利用抽签法纳入同日期接受冠脉造影的30例冠心病(coronary heart disease,CHD)患者和32例冠脉相对正常的受试者(对照组)。各组之间年龄、性别和其他基线特征基本平衡,通过流式细胞法检测外周血样中的淋巴细胞和单核细胞亚型。结果:CAE和CHD患者的外周血淋巴细胞亚型差异无统计学意义,但与CHD和对照组相比,CAE组的炎症型(非经典型)单核细胞比例显著增加[26.45%(16.90%~44.55%),13.70%(9.33%~17.60%),7.00%(13.70%~29.40%),P=0.000],经典型单核细胞比例显著降低[66.35%(39.73%~78.83%),82.90%(80.50%~89.40%),78.30%(56.70%~83.80%),P=0.000]。多重线性回归分析进一步证实了非经典单核细胞比例增加与CAE相关[定义CAE组=1,CHD组=2,对照组=3,故回归系数为负,即β=-0.371,P=0.000]。结论:CAE更可能是炎症性疾病,而不是免疫性疾病。
中图分类号:
刘锐锋, 盛倩倩, 张悦, 赵慧强. 冠状动脉扩张患者淋巴细胞和单核细胞亚型分析[J]. 内科理论与实践, 2022, 17(05): 373-378.
LIU Ruifeng, SHENG Qianqian, ZHANG Yue, ZHAO Huiqiang. Lymphocyte and monocyte subtypes in coronary artery ectasia patients[J]. Journal of Internal Medicine Concepts & Practice, 2022, 17(05): 373-378.
表1
研究对象的基线特征[n(%)/$\bar{x}±s$/M(Q1,Q3)]
| 指标 | 对照组(n=32) | CHD组(n=30) | CAE组(n=34) | F/χ2/Z | P |
|---|---|---|---|---|---|
| 年龄(岁) | 60.53±5.22 | 63.43±6.75 | 63.53±8.42 | 1.818 | 0.168 |
| 男性[n(%)] | 17(56.7) | 18(60.0) | 19(63.3) | 0.870 | 0.870 |
| 高血压[n(%)] | 21(70.0) | 26(86.7) | 26(86.7) | 0.174 | 0.174 |
| 收缩压(mmHg) | 121.30±13.04 | 129.28±19.51 | 124.57±14.6 | 1.870 | 0.160 |
| 舒张压(mmHg) | 72.83±8.47 | 77.14±19.19 | 75.37±11.94 | 0.720 | 0.490 |
| 糖尿病[n(%)] | 4(13.3) | 14(46.7) | 20(66.7) | 0.000 | 0.000 |
| 糖化血红蛋白(%) | 5.98±0.96 | 6.64±1.22 | 6.37±1.06 | 2.522 | 0.087 |
| 吸烟[n(%)] | 15(50.0) | 13(43.3) | 14(46.7) | 0.866 | 0.865 |
| 饮酒[n(%)] | 10(33.3) | 11(36.7) | 5(16.7) | 0.216 | 0.216 |
| CHD家族史[n(%)] | 5(16.6) | 12(40.0) | 9(30.0) | 0.134 | 0.134 |
| 高血压家族史[n(%)] | 8(26.7) | 14(46.7) | 7(23.3) | 0.127 | 0.127 |
| BMI(kg/m2) | 27.00(24.30, 29.00) | 26.30(23.81, 27.66) | 27.00(25.25, 28.07) | 0.413 | 0.285 |
| ALT(U/L) | 23.10(16.50, 27.50) | 18.00(13.00, 21.00) | 17.00(12.00, 32.00) | 2.916 | 0.066 |
| AST(U/L) | 19.60(16.00, 23.00) | 18.65(15.00, 23.00) | 18.70(17.35, 21.70) | 2.690 | 0.543 |
| 尿素氮(mmol/L) | 74.90(69.20, 89.50) | 82.80(70.50, 88.40) | 78.90(66.33, 91.53) | 0.193 | 0.796 |
| 血肌酐(μmol/L) | 4.82(4.16, 6.18) | 5.41(4.51, 6.27) | 5.07(4.13, 6.86) | 0.579 | 0.577 |
| TC(mmol/L) | 4.31(3.47, 4.79) | 3.85(3.36, 4.85) | 3.85(3.42, 4.84) | 0.075 | 0.743 |
| TG(mmol/L) | 1.40(0.88, 2.52) | 1.50(1.07, 1.82) | 1.42(1.04, 1.90) | 0.185 | 0.942 |
| HDL-C(mmol/L) | 1.11(0.87, 1.36) | 1.01(0.87, 1.28) | 0.95(0.82, 1.14) | 2.372 | 0.147 |
| LDL-C(mmol/L) | 2.25(1.73, 2.70) | 2.07(1.85, 2.60) | 2.06(1.77, 2.70) | 0.374 | 0.858 |
表2
3组患者炎症指标和冠脉造影特征[n(%)/ $\bar{x}±s$/M(Q1,Q3)]
| 指标 | 对照组(n=32) | CHD组(n=30) | CAE组(n=34) | F/χ2/Z | P |
|---|---|---|---|---|---|
| 白细胞(×109/L) | 6.52±1.43 | 7.22±2.02 | 6.72±1.37 | 1.455 | 0.239 |
| 淋巴细胞(×109/L) | 1.85±0.53 | 1.88±0.53 | 1.97±0.02 | 0.429 | 0.652 |
| 单核细胞(×109/L) | 0.42±0.12 | 0.41±0.13 | 0.41±0.13 | 0.001 | 0.999 |
| 中性粒细胞(×109/L) | 4.09±1.19 | 4.72±1.89 | 4.27±1.03 | 1.583 | 0.211 |
| NL比值 | 2.40±1.03 | 2.69±1.28 | 2.30±0.781 | 1.185 | 0.324 |
| 嗜碱性粒细胞(×109/L) | 0.04±0.02 | 0.04±0.02 | 0.04±0.02 | 0.292 | 0.747 |
| 嗜酸性粒细胞(×109/L) | 0.137±0.066 | 0.154±0.139 | 0.128±0.086 | 0.500 | 0.608 |
| hs-CRP(mg/L) | 1.29(0.46, 1.61) | 1.50(0.80, 3.07) | 1.30(0.68, 3.59) | 0.497 | 0.339 |
| ESR(mm/1h) | 7.00(4.00, 9.50) | 8.50(6.75, 12.25) | 9.00(6.00, 15.00) | 0.892 | 0.190 |
| 总胆红素(mmol/L) | 12.98(9.98, 16.00) | 12.63(10.30, 17.32) | 13.81(11.09, 17.91) | 0.776 | 0.470 |
| 直接胆红素(mmol/L) | 2.05(1.69, 3.13) | 2.52(1.69, 2.99) | 2.57(1.98, 3.38) | 0.092 | 0.685 |
| 间接胆红素(mmol/L) | 10.09(7.87, 14.21) | 10.03(7.79, 14.25) | 10.92(8.82, 14.18) | 0.344 | 0.452 |
| 左主干狭窄[n(%)] | - | 3(10.0) | 0(0.0) | 3.450 | 0.063 |
| 前降支狭窄[n(%)] | - | 25(83.3) | 29(85.3) | 0.249 | 0.618 |
| 回旋支狭窄[n(%)] | - | 21(70.0) | 19(55.9) | 0.964 | 0.326 |
| 右冠脉狭窄[n(%)] | - | 21(70.0) | 26(76.5) | 0.671 | 0.432 |
| Gensini评分 | - | 39.00(34.50, 54.00) | 36.50(31.00, 59.25) | -0.828 | 0.408 |
| 前降支的TFC(帧) | 28.00(23.00, 35.00) | 28.00(22.00, 39.00) | 39.50(33.00, 48.25) | 17.388 | 0.000 |
| 回旋支的TFC(帧) | 30.00(23.00, 33.00) | 25.00(19.00, 37.00) | 37.50(28.75, 52.25) | 11.098 | 0.000 |
| 右冠脉的TFC(帧) | 25.00(20.00, 30.00) | 21.00(18.00, 31.00) | 30.00(24.00, 44.00) | 10.529 | 0.002 |
| 左主干扩张[n(%)] | - | - | 7(20.6) | - | |
| 前降支扩张[n(%)] | - | - | 19(55.9) | - | |
| 回旋支扩张[n(%)] | - | - | 16(47.1) | - | |
| 右冠脉扩张[n(%)] | - | - | 26(76.5) | - |
表3
淋巴细胞亚群和单核细胞亚群分析[M(Q1,Q3),%]
| 指标 | 对照组(n=32) | CHD组(n=30) | CAE组(n=34) | P | P1 | P2 | P3 |
|---|---|---|---|---|---|---|---|
| CD3+CD4+淋巴细胞 | 41.10(26.70, 52.30) | 60.20(51.30, 72.83) | 58.30(47.45, 68.10) | 0.000 | 0.371 | 0.000 | 0.000 |
| CD3+CD8+淋巴细胞 | 24.30(18.10, 30.60) | 28.10(22.78, 34.65) | 31.25(23.23, 37.95) | 0.091 | 0.371 | 0.039 | 0.147 |
| CD16+淋巴细胞 | 13.20(8.35, 21.60) | 18.00(11.10, 21.70) | 14.90(10.53, 20.90) | 0.215 | 0.386 | 0.398 | 0.076 |
| CD19+淋巴细胞 | 3.02(1.30, 5.26) | 4.67(1.92, 6.70) | 3.02(1.81, 8.17) | 0.349 | 0.545 | 0.479 | 0.128 |
| 经典型单核细胞 | 78.30(56.70, 83.80) | 82.90(80.50, 89.40) | 66.35(39.73, 78.83) | 0.000 | 0.000 | 0.060 | 0.006 |
| 中间型单核细胞 | 1.03(0.35, 5.94) | 0.00(0.00, 0.00) | 1.47(0.22, 3.76) | 0.000 | 0.000 | 0.497 | 0.000 |
| 非经典型单核细胞 | 17.00(13.70, 29.40) | 13.70(9.33, 17.60) | 26.45(16.90, 44.55) | 0.000 | 0.000 | 0.046 | 0.015 |

图1
外周血单核细胞亚群分析 A:冠脉扩张组;B:CHD组;C:对照组。CD:白细胞分化抗原(cluster of differentiation)。单核细胞的3种亚型:经典型(CD14++CD16-)、中间型(CD14++CD16+)和非经典型(CD14+CD16++)。与CHD和对照组相比,CAE组的非经典单核细胞比例显著增加,经典型单核细胞比例显著下降。
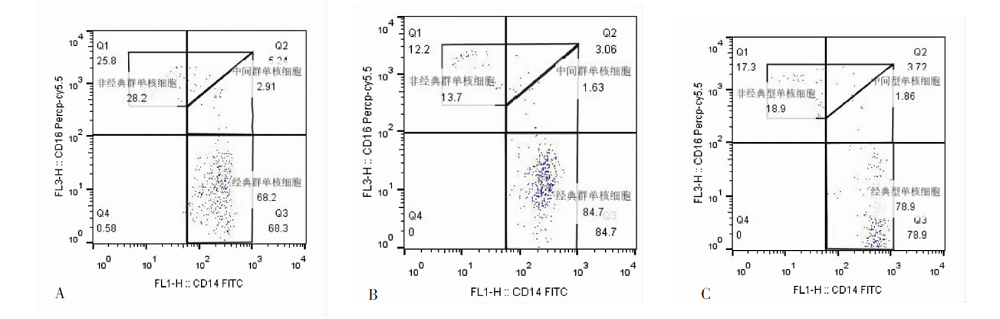
表4
以非经典型单核细胞为因变量进行多重线性回归
| 项目 | β | 95%置信区间 | 标准化β | t | P | |
|---|---|---|---|---|---|---|
| 常数 | 79.011 | 23.378 | 134.643 | 2.889 | 0.007 | |
| 组别(CAE组=1,CHD组=2,对照组=3) | -8.589 | -16.284 | -0.894 | -0.371 | -2.271 | 0.030 |
| 高血压(无=0, 有=1) | -24.608 | -42.003 | -7.214 | -0.494 | -2.878 | 0.007 |
| 中性粒细胞 | 4.650 | 1.095 | 8.205 | 0.412 | 2.661 | 0.012 |
| ESR | 0.732 | 0.124 | 1.339 | 0.386 | 2.451 | 0.020 |
| Gensini评分 | -0.278 | -0.556 | -0.001 | -0.332 | -2.040 | 0.049 |
| [1] |
Sheikh AS, Hailan A, Kinnaird T, et al. Coronary artery aneurysm: evaluation, prognosis, and proposed treatment strategies[J]. Heart Views, 2019, 20(3): 101-108.
doi: 10.4103/HEARTVIEWS.HEARTVIEWS_1_19 pmid: 31620255 |
| [2] |
Eitan A, Roguin A. Coronary artery ectasia: new insights into pathophysiology, diagnosis, and treatment[J]. Coron Artery Dis, 2016, 27(5): 420-428.
doi: 10.1097/MCA.0000000000000379 URL |
| [3] |
Markis JE, Joffe CD, Cohn PF, et al. Clinical significance of coronary arterial ectasia[J]. Am J Cardiol, 1976, 37(2): 217-222.
pmid: 1108631 |
| [4] |
Li JJ, He JG, Nan JL, et al. Is systemic inflammation responsible for coronary artery ectasia?[J]. Int J Cardiol, 2008, 130(2): e69-e70.
doi: 10.1016/j.ijcard.2007.11.078 URL |
| [5] |
Balta S, Demir M, Ozturk C, et al. The relation between inflammation and coronary artery ectasia[J]. Rev Port Cardiol, 2016, 35(10): 553-554.
doi: 10.1016/j.repc.2016.04.011 pmid: 27637373 |
| [6] |
Huang W, Berube J, McNamara M, et al. Lymphocyte subset counts in COVID-19 patients[J]. Cytometry A, 2020, 97(8): 772-776.
doi: 10.1002/cyto.a.24172 URL |
| [7] |
Cormican S, Griffin MD. Human monocyte subset distinctions and function[J]. Front Immunol, 2020, 11: 1070.
doi: 10.3389/fimmu.2020.01070 pmid: 32582174 |
| [8] |
Tamis-Holland JE, Jneid H, Reynolds HR, et al. Contemporary diagnosis and management of patients with myocardial infarction in the absence of obstructive coronary artery disease[J]. Circulation, 2019, 139(18): e891-e908.
doi: 10.1161/CIR.0000000000000670 |
| [9] |
Lin JP, Vitek L, Schwertner HA. Serum bilirubin and genes controlling bilirubin concentrations as biomarkers for cardiovascular disease[J]. Clin Chem, 2010, 56(10): 1535-1543.
doi: 10.1373/clinchem.2010.151043 URL |
| [10] | Tsai WN, Wang YY, Liang JT, et al. Serum total bilirubin concentrations are inversely associated with total white blood cell counts in an adult population[J]. Ann Clin Biochem, 2015, 52 Pt2: 251-258. |
| [11] |
Turhan H, Erbay AR, Yasar AS, et al. Impaired coronary blood flow in patients with metabolic syndrome[J]. Am Heart J, 2004, 148(5): 789-794.
pmid: 15523308 |
| [12] | 李彭军, 韩慧文, 葛兰, 等. 健康体检者循环单核细胞亚群与性别及年龄的关系[J]. 武警医学, 2014, 25(1): 5-8. |
| [13] |
Chen J, Zhang Y, Liu J, et al. Role of lipoprotein(a) in predicting the severity of new on-set coronary artery disease in type 2 diabetics[J]. Diab Vasc Dis Res, 2015, 12(4): 258-264.
doi: 10.1177/1479164115579004 URL |
| [14] | Matta AG, Yaacoub N, Nader V, et al. Coronary artery aneurysm[J]. World J Cardiol, 2021, 26, 13(9): 446-455. |
| [15] |
Sheikh AS, Hailan A, Kinnaird T, et al. Coronary artery aneurysm: evaluation, prognosis, and proposed treatment strategies[J]. Heart Views, 2019, 20(3): 101-108.
doi: 10.4103/HEARTVIEWS.HEARTVIEWS_1_19 pmid: 31620255 |
| [16] |
Virmani R, Robinowitz M, Atkinson JB, et al. Acquired coronary arterial aneurysms[J]. Hum Pathol, 1986, 17(6): 575-583.
pmid: 3710470 |
| [17] |
Sarli B, Baktir AO, Saglam H, et al. Neutrophil-to-lymphocyte ratio is associated with severity of coronary artery ectasia[J]. Angiology, 2014, 65(2): 147-151.
doi: 10.1177/0003319713488932 pmid: 23657176 |
| [18] |
Li JJ, Nie SP, Qian XW, et al. Chronic inflammatory status in patients with coronary artery ectasia[J]. Cytokine, 2009, 46(1): 61-64.
doi: 10.1016/j.cyto.2008.12.012 URL |
| [19] |
Iwańczyk S, Borger M, Kamiński M, et al. Inflammatory response in patients with coronary artery ectasia and coronary artery disease[J]. Kardiol Pol, 2019, 77(7-8): 713-715.
doi: 10.33963/KP.14812 pmid: 31066726 |
| [20] |
Lamblin N, Bauters C, Hermant X, et al. Polymorphisms in the promoter regions of MMP-2, MMP-3, MMP-9 and MMP-12 genes as determinants of aneurysmal coronary artery disease[J]. J Am Coll Cardiol, 2002, 40(1): 43-48.
pmid: 12103254 |
| [21] |
Finkelstein A, Michowitz Y, Abashidze A, et al. Temporal association between circulating proteolytic, inflammatory and neurohormonal markers in patients with coronary ectasia[J]. Atherosclerosis, 2005, 179(2): 353-359.
pmid: 15777553 |
| [22] |
Lee NY, Park HY, Park CK, et al. Analysis of systemic endothelin-1, matrix metalloproteinase-9, macrophage chemoattractant protein-1, and high-sensitivity C-reactive protein in normal-tension glaucoma[J]. Curr Eye Res, 2012, 37(12): 1121-1126.
doi: 10.3109/02713683.2012.725798 pmid: 22966842 |
| [23] |
Liu R, Chen L, Wu W, et al. Neutrophil serine proteases and their endogenous inhibitors in coronary artery ectasia patients[J]. Anatol J Cardiol, 2016, 16(1): 23-28.
doi: 10.5152/akd.2015.6072 pmid: 26467359 |
| [24] |
Katritsis DG, Zografos T, Korovesis S, et al. Antiendothelial cell antibodies in patients with coronary artery ectasia[J]. Coron Artery Dis, 2010, 21(16): 352-356.
doi: 10.1097/MCA.0b013e32833d5fae URL |
| [1] | 李士杰 姜爱莉 刘宇 王召旭 韩倩倩. 巨噬细胞介导的炎症反应在材料生物相容性评价中的意义[J]. 组织工程与重建外科杂志, 2022, 18(5): 436-. |
| [2] | 闫晓红, 薄建萍. 呼出气一氧化氮在下气道慢性炎症疾病中的评估价值[J]. 内科理论与实践, 2022, 17(05): 418-422. |
| [3] | 刘萍, 肖园, 王歆琼, 陆亭伟, 赵雪松, 杨媛艳. Wiskott-Aldrich综合征合并克罗恩病一例并文献复习[J]. 诊断学理论与实践, 2022, 21(03): 349-354. |
| [4] | 戴生明. 银屑病关节炎的诊治现状与挑战[J]. 内科理论与实践, 2022, 17(03): 186-189. |
| [5] | 张磊, 毛家玺, 李涛, 滕飞, 孙克彦. 术前免疫炎症反应对原发性胆汁性胆管炎肝移植病人预后影响的双中心回顾性研究[J]. 外科理论与实践, 2022, 27(02): 158-164. |
| [6] | 王毅, 李红鹏, 张力月, 李庆云. 瘦素与重度哮喘的关联及机制研究进展[J]. 内科理论与实践, 2022, 17(01): 88-91. |
| [7] | 朱秋艳, 薛岑. 半胱氨酸蛋白酶抑制剂C在呼吸系统疾病中的研究进展[J]. 内科理论与实践, 2022, 17(01): 102-106. |
| [8] | 雷晓旭 王春 赵曦. 炎症微环境作用下 BMPs-ERK5 信号通路对牙周膜干细胞成骨分化的影响 #br#[J]. 组织工程与重建外科杂志, 2021, 17(1): 30-. |
| [9] | 王虎, 张姣姣, 孙俊楠, 王海嵘. 白介素-6联合CD4+T淋巴细胞百分比对脓毒症患者预后的评估价值[J]. 内科理论与实践, 2021, 16(06): 404-408. |
| [10] | 宋娟, 邢寅, 黄慧, 陆帅, 秦利. 上海市崇明地区中老年人群血白细胞计数与血尿酸水平相关性研究[J]. 内科理论与实践, 2021, 16(06): 413-417. |
| [11] | 王常刚, 刘坤, 冯浩然, 蒋奕玫, 施毅卿, 陈献则, 宋子甲, 李军, 李佑, 蔡东莉, 赵任. 结肠直肠癌B7S1表达与免疫浸润的关系[J]. 外科理论与实践, 2021, 26(04): 336-342. |
| [12] | 查晴, 于晨溪, 刘亚, 杨玲, 叶佳雯, 刘艳. miR-16在冠状动脉粥样硬化斑块进展中的作用及初步机制研究[J]. 诊断学理论与实践, 2021, 20(01): 82-87. |
| [13] | 崔基浩, 李创, 马文斌, 李春, 徐万宏. 自体骨髓单核细胞移植对兔退行性病变后椎间盘的修复作用[J]. 组织工程与重建外科杂志, 2020, 16(3): 237-240. |
| [14] | 刘冰滢, 王文波, 黄佳, 高振, 武晓莉, 刘伟. 积雪草酸葡糖胺盐凝胶通过调节巨噬细胞迁移和极化促进创面愈合及表皮再生[J]. 组织工程与重建外科杂志, 2020, 16(2): 112-118. |
| [15] | 程雨龙, 杨松林, 邓辰亮, 郑江红. 桃叶珊瑚苷抑制机械张力诱导增生性瘢痕的机制研究[J]. 组织工程与重建外科杂志, 2020, 16(2): 119-122. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||