内科理论与实践 ›› 2024, Vol. 19 ›› Issue (01): 51-56.doi: 10.16138/j.1673-6087.2024.01.09
舒扬1a,2, 贺晓双1a, $\boxed{\hbox{陈虹}}$1b, 时国朝1b, 方洁1a( )
)
收稿日期:2023-09-15
出版日期:2024-02-29
发布日期:2024-04-28
通讯作者:
方洁
E-mail:fj40517@rjh.com.cn
基金资助:
SHU Yang1a,2, HE Xiaoshuang1a, $\boxed{\hbox{CHEN Hong}}$1b, SHI Guochao1b, FANG Jie1a()
Received:2023-09-15
Online:2024-02-29
Published:2024-04-28
Contact:
FANG Jie
E-mail:fj40517@rjh.com.cn
摘要:
目的: 探索监测复方磺胺甲噁唑(sulfamethoxazole complex, SMZco)中SMZ血药峰浓度对接受SMZco片治疗的非人类免疫缺陷病毒(immunodeficiency virus, HIV)感染患者耶氏肺孢子菌肺炎(Pneumocystis jirovecii pneumonia,PJP)疗效和安全性的指导意义。方法: 采集2019年1月至2023年5月在瑞金医院住院治疗的非HIV PJP患者的临床数据,回顾性分析患者SMZ血药峰浓度与疗效和不良反应发生情况的关系。结果: 共纳入47例患者,SMZ的血药峰浓度范围为87.49~334.31 mg/L,中位数(四分位间距)为168.62(79.72) mg/L,64%的患者血药峰浓度>150 mg/L。患者30 d全因死亡率为28%,治疗阳性反应率为66%。其中,SMZ血药峰浓度≤150 mg/L患者与>150 mg/L患者30 d全因死亡和治疗阳性反应率差异无统计学意义。29例(62%)患者发生不良反应。相比SMZ血药峰浓度≤150 mg/L的患者,>150 mg/L的患者血小板减少(40%比6%,P=0.025)和血红蛋白降低(37%比0,P=0.013)等不良反应发生率更高,且严重不良反应的发生率更高(43%比12%,P=0.026)。结论: SMZco片用于治疗非HIV PJP患者时,SMZ血药峰浓度≤150 mg/L的患者较>150 mg/L的患者可获得相当的疗效,且发生严重不良反应的风险更小,建议该类患者常规监测SMZ血药峰浓度。
中图分类号:
舒扬, 贺晓双, $\boxed{\hbox{陈虹}}$, 时国朝, 方洁. 复方磺胺甲噁唑血药峰浓度测定对治疗非人类免疫缺陷病毒感染患者耶氏肺孢子菌肺炎的临床意义[J]. 内科理论与实践, 2024, 19(01): 51-56.
SHU Yang, HE Xiaoshuang, $\boxed{\hbox{CHEN Hong}}$, SHI Guochao, FANG Jie. Clinical significance of plasma peak concentration determination of compound sulfamethoxazole in treatment of Pneumocystis jirovecii pneumonia in patients with non-human immunodeficiency virus infection[J]. Journal of Internal Medicine Concepts & Practice, 2024, 19(01): 51-56.
表1
非HIV感染PJP患者基本资料[$\bar{x} \pm s$/n(%)/M(IQR)]
| 项目 | 全部患者(n=47) | SMZ峰浓度≤150 mg/L(n=17) | SMZ峰浓度>150 mg/L(n=30) | t/χ2/Z | P |
|---|---|---|---|---|---|
| 年龄(岁) | 57.62±15.65 | 58.59±14.88 | 56.67±15.78 | 0.622 | 0.537 |
| 男性[n(%)] | 24(51) | 10(59) | 14(47) | 0.642 | 0.423 |
| 体质量指数(kg/m2) | 21.98±3.68 | 22.73±4.03 | 21.54±3.46 | 1.065 | 0.992 |
| 发热[n(%)] | 29(62) | 12(71) | 13(57) | 0.890 | 0.345 |
| 有创机械通气[n(%)] | 14(32) | 5(29) | 9(33) | 0.074 | 0.786 |
| 白细胞计数(×109/L) | 7.65(5.97) | 6.05(5.53) | 8.04(4.93) | -1.528 | 0.127 |
| 淋巴细胞计数(×109/L) | 0.50(0.48) | 0.48(0.63) | 0.47(0.46) | -0.833 | 0.406 |
| 乳酸脱氢酶(μmol/L) | 458(297.25) | 475.00(323.00) | 458.00(184.25) | -0.231 | 0.818 |
| G试验(pg/mL) | 194.71(380.39) | 260.53(549.06) | 199.03(245.77) | -0.764 | 0.445 |
| CD4+T细胞(/μL) | 170.00(279.00) | 286.00(309.00) | 125.00(184.00) | -1.674 | 0.094 |
| 氧分压(mmHg) | 71(30.50) | 71.00(33.00) | 69.00(29) | -0.308 | 0.758 |
| 二氧化碳分压(mmHg) | 35(8.00) | 35.00(8.00) | 34.00(8.00) | -0.915 | 0.360 |
| 自身免疫性疾病[n(%)] | 32(68) | 13(76) | 19(63) | 0.862 | 0.353 |
| 恶性肿瘤[n(%)] | 18(38) | 6(35) | 12(40) | 0.102 | 0.750 |
| 间质性肺病[n(%)] | 10(20) | 1(6) | 9(30) | 2.466 | 0.116 |
| 高血压病[n(%)] | 10(20) | 2(12) | 8(27) | 0.687 | 0.407 |
| 糖尿病[n(%)] | 9(19) | 4(24) | 5(17) | 0.036 | 0.850 |
| 合并感染[n(%)] | 32(68) | 11(65) | 21(70) | 0.140 | 0.708 |
| 合并细菌感染[n(%)] | 27(57) | 9(53) | 18(60) | 0.221 | 0.638 |
| 合并其他真菌感染[n(%)] | 13(28) | 5(29) | 8(27) | 0.000 | 1.000 |
| 合并使用抗菌药物[n(%)] | 46(98) | 16(94) | 30(100) | 0.085 | 0.771 |
| 合并使用卡泊芬净[n(%)] | 29(62) | 9(53) | 20(67) | 0.865 | 0.352 |
表2
非HIV感染PJP患者30 d全因死亡率和治疗阳性反应率[n(%)]
| 项目 | 全部患者(n=47) | SMZ峰浓度≤150 mg/L(n=17) | SMZ峰浓度>150 mg/L(n=30) | χ2 | P |
|---|---|---|---|---|---|
| 30 d全因死亡率 | 13(28) | 4(24) | 9(30) | 0.019 | 0.891 |
| 治疗阳性反应率 | 31(66) | 12(71) | 19(63) | 0.254 | 0.614 |
表2
SMZ起始给药剂量及血药峰浓度测定[$\bar{x} \pm s$/n(%)/M(IQR)]
| 项目 | 全部患者 (n=47) | SMZ峰浓度≤150 mg/L (n=17) | SMZ峰浓度>150 mg/L (n=30) | t/χ2/Z | P |
|---|---|---|---|---|---|
| 初始给药剂量[mg/(kg·d)] | 61.73±19.02 | 53.89±17.68 | 66.17±18.56 | -2.215 | 0.785 |
| SMZ-TMP给药剂量小于说明书推荐下限[n(%)] | 37(79) | 15(88) | 22(73) | 0.687 | 0.407 |
| 肾小球滤过率(mL/min) | 95.13(52.58) | 85.08(70.82) | 97.84(49.30) | -1.816 | 0.069 |

图1
SMZ起始给药剂量与血药峰浓度的关系
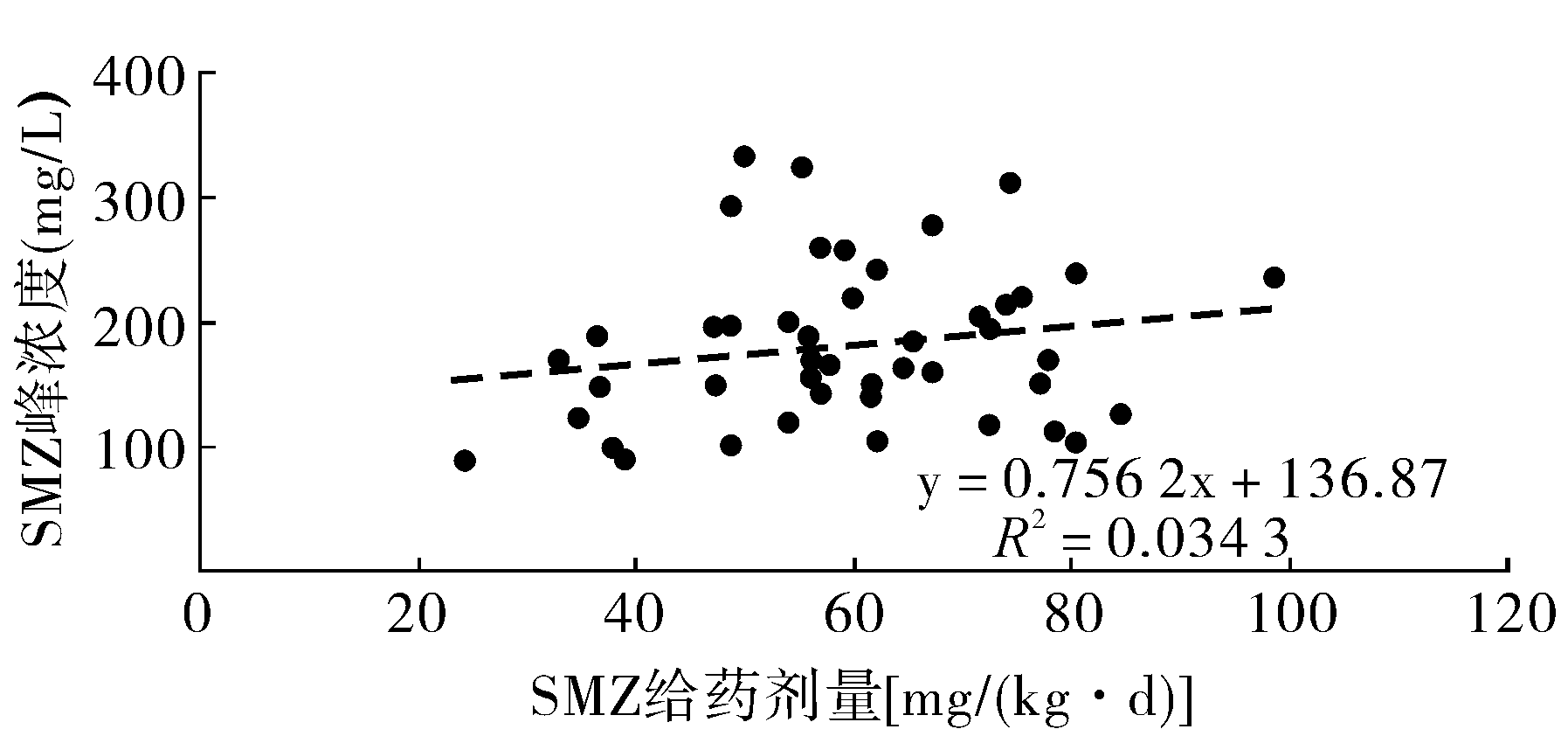
表4
SMZ血药峰浓度与不良反应发生率的关系[n(%)]
| 项目 | 总例数 (n=47) | SMZ峰浓度 >150 mg/L (n=30) | SMZ峰浓度 ≤150 mg/L (n=17) | χ2 | P |
|---|---|---|---|---|---|
| 不良反应 | 29(62) | 21(70) | 8(47) | 2.417 | 0.120 |
| 血小板减少 | 13(28) | 12(40) | 1(6) | 5.025 | 0.025 |
| 血红蛋白下降 | 11(23) | 11(37) | 0(0) | 6.221 | 0.013 |
| 转氨酶异常 | 10(21) | 7(23) | 3(18) | 0.008 | 0.931 |
| 胃肠道反应 | 8(17) | 5(17) | 3(18) | 0.000 | 1.000 |
| 胆红素升高 | 6(13) | 4(13) | 2(12) | 0.000 | 1.000 |
| 肌酐升高 | 4(9) | 4(13) | 0(0) | 1.125 | 0.289 |
| 中性粒减少 | 3(6) | 2(7) | 1(6) | 0.000 | 1.000 |
| 严重不良反应 | 15(32) | 13(43) | 2(12) | 4.977 | 0.026 |
| 血红蛋白下降 | 6(13) | 6(20) | 0(0) | 2.309 | 0.129 |
| 血小板减少 | 5(11) | 5(17) | 0(0) | 1.660 | 0.198 |
| 转氨酶异常 | 4(9) | 4(13) | 0(0) | 1.061 | 0.303 |
| 胆红素升高 | 4(9) | 2(7) | 2(12) | 0.003 | 0.954 |
| [1] |
Tokuda H, Sakai F, Yamada H, et al. Clinical and radiological features of Pneumocystis pneumonia in patients with rheumatoid arthritis, in comparison with methotrexate Pneumonitis and Pneumocystis pneumonia in acquired immunodeficiency syndrome[J]. Intern Med, 2008, 47(10):915-923.
doi: 10.2169/internalmedicine.47.0702 URL |
| [2] |
Thomas CF Jr, Limper AH. Pneumocystis pneumonia[J]. N Engl J Med, 2004, 350(24):2487-2498.
doi: 10.1056/NEJMra032588 URL |
| [3] |
Maschmeyer G, Helweg-Larsen J, Pagano L, et al. ECIL guidelines for treatment of Pneumocystis jirovecii pneumonia in non-HIV-infected haematology patients[J]. J Antimicrob Chemother, 2016, 71(9):2405-2413.
doi: 10.1093/jac/dkw158 pmid: 27550993 |
| [4] | Fishman JA, Gans H. Pneumocystis jiroveci in solid organ transplantation[J]. Clin Transplant, 2019, 33(9):e13587. |
| [5] |
Chang HM, Tsai HC, Lee SS, et al. High daily doses of trimethoprim/sulfamethoxazole are an independent risk factor for adverse reactions in patients with Pneumocystis pneumonia and AIDS[J]. J Chin Med Assoc, 2016, 79(6):314-319.
doi: 10.1016/j.jcma.2016.01.007 URL |
| [6] |
Hughes WT, Feldman S, Chaudhary SC, et al. Comparison of pentamidine isethionate and trimethoprim-sulfamethoxazole in the treatment of Pneumocystis carinii pneumonia[J]. J Pediatr, 1978, 92(2):285-291.
doi: 10.1016/S0022-3476(78)80028-6 URL |
| [7] |
Chin TW, Vandenbroucke A, Fong IW. Pharmacokinetics of trimethoprim-sulfamethoxazole in critically ill and non-critically ill AIDS patients[J]. Antimicrob Agents Chemother, 1995, 39(1):28-33.
doi: 10.1128/AAC.39.1.28 pmid: 7695325 |
| [8] |
Kim T, Hong HL, Lee YM, et al. Is caspofungin really an effective treatment for Pneumocystis jirovecii pneumonia in immunocompromised patients without human immunodeficiency virus infection?[J]. Scand J Infect Dis, 2013, 45(6):484-488.
doi: 10.3109/00365548.2012.760842 URL |
| [9] | 潘欢妍, 祁慧, 梁培, 等. 重症耶氏肺孢子菌肺炎患者复方磺胺甲噁唑血药浓度监测的临床研究[J]. 中南药学, 2023, 21(6):1653-1658. |
| [10] | Kosaka M, Ushiki A, Ikuyama Y, et al. A four-center retrospective study of the efficacy and toxicity of low-dose trimethoprim-sulfamethoxazole for the treatment of Pneumocystis pneumonia in patients without HIV infection[J]. Antimicrob Agents Chemother, 2017, 61(12):e01173-e01217. |
| [11] |
Nakashima K, Aoshima M, Nakashita T, et al. Low-dose trimethoprim-sulfamethoxazole treatment for Pneumocystis pneumonia in non-human immunodeficiency virus-infected immunocompromised patients[J]. J Microbiol Immunol Infect, 2018, 51(6):810-820.
doi: S1684-1182(17)30147-0 pmid: 28779879 |
| [12] |
Ohmura SI, Naniwa T, Tamechika SY, et al. Effectiveness and safety of lower dose sulfamethoxazole/trimethoprim therapy for Pneumocystis jirovecii pneumonia in patients with systemic rheumatic diseases[J]. J Infect Chemother, 2019, 25(4):253-261.
doi: 10.1016/j.jiac.2018.11.014 URL |
| [13] |
Chin TW, Vandenbroucke A, Fong IW. Pharmacokinetics of trimethoprim-sulfamethoxazole in critically ill and non-critically ill AIDS patients[J]. Antimicrob Agents Chemother, 1995, 39(1):28-33.
doi: 10.1128/AAC.39.1.28 pmid: 7695325 |
| [14] |
Hall RG Nd, Pasipanodya JG, Meek C, et al. Fractal geometry-based decrease in trimethoprim-sulfamethoxazole concentrations in overweight and obese people[J]. CPT Pharmacometrics Syst Pharmacol, 2016, 5(12):674-681.
doi: 10.1002/psp4.v5.12 URL |
| [15] | Reeves DS, Wilkinson PJ. The pharmacokinetics of trimethoprim and trimethoprim/sulphonamide combinations, including penetration into body tissues[J]. Infection, 1979, 7 Suppl 4:S330-S341. |
| [16] |
Kagaya H, Miura M, Niioka T, et al. Influence of NAT2 polymorphisms on sulfamethoxazole pharmacokinetics in renal transplant recipients[J]. Antimicrob Agents Chemother, 2012, 56(2):825-829.
doi: 10.1128/AAC.05037-11 pmid: 22106207 |
| [17] | Kavanagh ON. Alkalising agents in urinary tract infections: theoretical contraindications, interactions and synergy[J]. Ther Adv Drug Saf, 2022, 13:20420986221080794. |
| [1] | 何敏敏, 茅越丽. 延续性护理对透明质酸注射美容后不良反应的影响分析 [J]. 组织工程与重建外科杂志, 2024, 20(3): 351-. |
| [2] | 方洁, 陈超, 周敏. 对耶氏肺孢子菌肺炎患者进行复方磺胺甲噁唑治疗药物监测的重要性研究[J]. 内科理论与实践, 2024, 19(01): 31-36. |
| [3] | 周芮, 吴涛, 薛锋, 田红娟, 刘文慧, 毛东锋. 达雷妥尤单抗治疗复发/难治性多发性骨髓瘤疗效及安全性分析[J]. 内科理论与实践, 2023, 18(05): 348-351. |
| [4] | 李洵桦. 肝豆状核变性的内科治疗[J]. 内科理论与实践, 2021, 16(05): 289-293. |
| [5] | 王晓斐, 张秋蕊. 免疫检查点抑制剂致肺部不良反应的诊治进展[J]. 诊断学理论与实践, 2021, 20(04): 343-348. |
| [6] | 顾卫琼. 免疫检查点抑制剂致甲状腺损伤的诊治进展[J]. 诊断学理论与实践, 2021, 20(04): 338-342. |
| [7] | 游碧君, 王金辉, 庄鸿源. 儿童输血反应发生率及输血反应原因分析和改进措施探讨[J]. 诊断学理论与实践, 2021, 20(04): 396-398. |
| [8] | 沈悦,张懿,徐晶,刘武林. 强脉冲光(420 nm+560 nm)联合无针水光治疗难治性痤疮的临床疗效[J]. 组织工程与重建外科杂志, 2019, 15(2): 95-97. |
| [9] | 程毅敏, 庄衍, 杭海芳, 窦红菊,. 探讨利妥昔单抗联合CHOP方案治疗弥漫大B细胞淋巴瘤的临床疗效[J]. 内科理论与实践, 2019, 14(05): 317-318. |
| [10] | 康健捷, 杨红军, 邓兵梅, 邵腾飞. 利福平致药源性流感样综合征一例临床分析[J]. 诊断学理论与实践, 2018, 17(04): 460-461. |
| [11] | 戴强,施文娟,陈晓明,徐琦量. 透明质酸填充改善面部皱纹的临床疗效[J]. 组织工程与重建外科杂志, 2016, 12(6): 371-380. |
| [12] | 张仁芳, 刘莉, 沈银忠, 王江蓉, 齐唐凯, 汤阳, 宋炜, 王珍燕, 卢洪洲,. 抗病毒治疗并发严重不良反应后更换洛匹那韦/利托那韦片的疗效观察[J]. 内科理论与实践, 2016, 11(05): 269-272. |
| [13] | 金燕萍, 朱敏华, 江铭. 临床输血不良反应情况分析及预防措施探讨[J]. 诊断学理论与实践, 2016, 15(05): 503-506. |
| [14] | 龚邦东, 张晓宇, 程昉, 冯润, 房星星, 汤建平,. 白芍总苷联合小剂量沙利度胺治疗原发性干燥综合征的安全性和疗效[J]. 内科理论与实践, 2015, 10(02): 108-111. |
| [15] | 窦汉波, 罗炎, 樊星, 王苓, 唐暐, 胡炯,. 大剂量阿糖胞苷巩固治疗核心结合因子相关急性髓系白血病的疗效及安全性分析[J]. 内科理论与实践, 2013, 8(06): 423-426. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||