内科理论与实践 ›› 2021, Vol. 16 ›› Issue (06): 404-408.doi: 10.16138/j.1673-6087.2021.06.007
王虎, 张姣姣, 孙俊楠, 王海嵘( )
)
收稿日期:2021-03-18
出版日期:2021-12-27
发布日期:2022-07-25
通讯作者:
王海嵘
E-mail:drwhr75@163.com
WANG Hu, ZHANG Jiaojiao, SUN Junnan, WANG Hairong()
Received:2021-03-18
Online:2021-12-27
Published:2022-07-25
Contact:
WANG Hairong
E-mail:drwhr75@163.com
摘要:
目的:评估白介素-6(interleukin-6,IL-6)联合CD4+T淋巴细胞百分比对脓毒症患者预后的价值。方法:收集2016年6月至2019年6月我院急诊医学科158例脓毒症患者资料,如入院24 h内IL-6、CD4+T淋巴细胞百分比、CD4+T淋巴细胞、C反应蛋白(C-reactive protein, CRP)、降钙素原(procalcitonin, PCT)、人白细胞DR抗原(human leukocyte DR antigen, HLA-DR),以及计算患者的脓毒症相关性器官功能衰竭评价(sepsis-related organ failure assessment,SOFA)评分、急性生理和慢性健康状况评价Ⅱ(acute physiology and chronic health evaluation-Ⅱ,APACHEⅡ)评分,根据28 d预后情况分为存活组和死亡组,比较2组SOFA评分、APACHEⅡ评分、IL-6、CD4+T淋巴细胞百分比、CD4+T淋巴细胞、CRP、PCT、HLA-DR的差异,分析IL-6、CD4+T淋巴细胞百分比与APACHEⅡ评分、SOFA评分的相关性,绘制受试者操作特征(receiver operating characteristic, ROC)曲线,评估以上各因素、IL-6、CD4+T淋巴细胞百分比及两者联合对脓毒症预后的判断价值。结果:死亡组APACHEⅡ评分(t=4.514,P<0.001)、SOFA评分(t=4.711,P<0.001)、IL-6(Z=2.114,P=0.035)、PCT(t=2.192,P=0.021)、CRP(Z=2.208,P=0.033)、D-二聚体(Z=1.963,P=0.043)高于存活组;死亡组CD4+T淋巴细胞百分比(Z=2.398,P=0.016)、HLA-DR(t=2.004,P=0.040)较存活组显著降低。将IL-6、CD4+T淋巴细胞百分比与APACHEⅡ评分、SOFA评分进行Spearman相关性分析,结果显示IL-6与APACHEⅡ评分、SOFA评分呈正相关(r=0.351、0.478,均P<0.05),CD4+T淋巴细胞百分比与APACHEⅡ评分、SOFA评分呈负相关(r=-0.347、-0305,均P<0.05)。ROC曲线示IL-6联合 CD4+T淋巴细胞百分比的曲线下面积(area under the curve, AUC)(0.793,P<0.001)最高,灵敏度为86.7%,特异度为63.0%,两因素联合的预测效果较单一指标更好。结论:IL-6联合CD4+T淋巴细胞百分比是判断脓毒症的预后的因素,两因素联合较单一指标评估效果更佳。
中图分类号:
王虎, 张姣姣, 孙俊楠, 王海嵘. 白介素-6联合CD4+T淋巴细胞百分比对脓毒症患者预后的评估价值[J]. 内科理论与实践, 2021, 16(06): 404-408.
WANG Hu, ZHANG Jiaojiao, SUN Junnan, WANG Hairong. Evaluating value of interleukin-6 combined with CD4+ T cell percentage on prognosis in patients with sepsis[J]. Journal of Internal Medicine Concepts & Practice, 2021, 16(06): 404-408.
表1
研究受试者的基线临床特征和实验室检查特征[$\bar{x}±s$/n(%)/M(Q1,Q3)]
| 项目 | 存活组(n=127) | 死亡组(n=31) | t/χ2/Z | P |
|---|---|---|---|---|
| 男性[n(%)] | 66(52.0) | 18(58.1) | 0.372 | 0.542 |
| 年龄(岁) | 71.17±16.72 | 76.23±10.74 | 1.602 | 0.111 |
| APACHEⅡ评分(分) | 15.39±6.12 | 21.19±5.94 | 4.514 | <0.001 |
| SOFA评分(分) | 5.23±2.94 | 8.71±3.72 | 4.711 | <0.001 |
| 基础疾病[n(%)] | ||||
| 高血压病 | 73(57.5) | 14(45.2) | 1.528 | 0.216 |
| 糖尿病 | 36(28.3) | 5(16.1) | 1.936 | 0.164 |
| 冠心病 | 50(39.4) | 14(45.2) | 0.347 | 0.556 |
| 脑血管疾病 | 25(19.7) | 5(16.1) | 0.205 | 0.651 |
| 慢性肾脏病 | 14(11.0) | 3(9.7) | 0.047 | 1.000 |
| 原发疾病[n(%)] | ||||
| 肺炎 | 51(40.2) | 14(45.1) | - | - |
| 消化系统感染 | 21(16.5) | 6(19.4) | - | - |
| 泌尿系统感染 | 14(11.0) | 3(9.7) | - | - |
| 颅内感染 | 11(8.7) | 3(9.7) | - | - |
| 其他 | 30(23.6) | 5(16.1) | - | - |
| PCT(mg/L) | 11.09±1.49 | 24.59±3.90 | 2.192 | 0.021 |
| CRP(mg/L) | 122.00(62.00,174.00) | 160.00(73.00,196.00) | 2.208 | 0.033 |
| IL-6(ng/L) | 34.70(15.85,84.70) | 138.50(14.50,861.00) | 2.114 | 0.035 |
| HLA-DR | 1 865.38±601.41 | 1 206.74±633.32 | 2.004 | 0.040 |
| D-二聚体(mg/L) | 1.17(0.73,2.64) | 2.86(1.13,5.95) | 1.963 | 0.043 |
| CD4+T淋巴细胞(个/μL) | 271.8(172.5,432.3) | 193.0(84.0,359.0) | 1.827 | 0.068 |
| CD4+T细胞百分比(%) | 38.07(31.80,45.36) | 31.10(19.95,37.50) | 2.398 | 0.016 |
表2
IL-6、CD4+T淋巴细胞百分比与SOFA评分相关性分析
| 指标 | APACHEⅡ评分 | SOFA评分 | |||
|---|---|---|---|---|---|
| r | P | r | P | ||
| IL-6 | 0.351 | 0.024 | 0.478 | <0.001 | |
| CD4+T淋巴细胞百分比 | -0.347 | 0.031 | -0.305 | 0.043 | |
图1
受试者ROC曲线
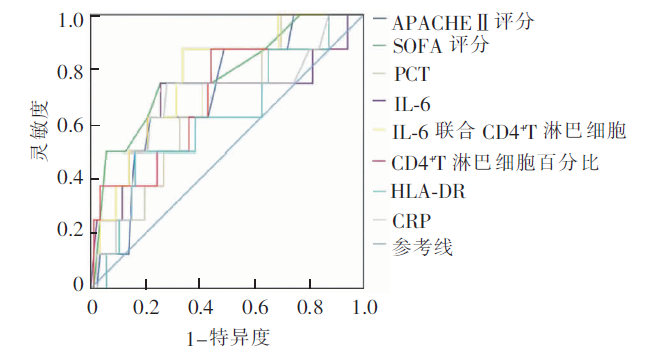
表3
各变量评估脓毒症患者死亡风险效果
| 变量 | AUC | P | 95%CI | 截断值 | 灵敏度(%) | 特异度(%) |
|---|---|---|---|---|---|---|
| SOFA评分 | 0.750 | 0.002 | 0.610~0.890 | 5.5 | 80.0 | 63.0 |
| APACHEⅡ评分 | 0.732 | 0.004 | 0.601~0.862 | 18.5 | 66.7 | 72.2 |
| CD4+T淋巴细胞百分比 | 0.673 | 0.030 | 0.505~0.841 | 35.9 | 80.1 | 55.6 |
| IL-6 | 0.683 | 0.015 | 0.520~0.867 | 68.1 | 73.3 | 71.3 |
| PCT | 0.694 | 0.011 | 0.505~0.861 | 17.7 | 75.1 | 65.3 |
| CRP | 0.675 | 0.038 | 0.470~0.896 | 137.0 | 74.3 | 61.8 |
| HLA-DR | 0.624 | 0.149 | 0.416~0.832 | 1 498.5 | 50.0 | 83.7 |
| IL-6联合CD4+T细胞百分比 | 0.793 | <0.001 | 0.684~0.901 | 0.1 | 86.7 | 63.0 |
| [1] |
Cecconi M, Evans L, Levy M, et al. Sepsis and septic shock[J]. Lancet, 2018, 392(10141): 75-87.
doi: 10.1016/S0140-6736(18)30696-2 URL |
| [2] |
Peters van Ton AM, Kox M, Abdo WF, et al. Precision immunotherapy for sepsis[J]. Front Immunol, 2018, 9: 1926.
doi: 10.3389/fimmu.2018.01926 URL |
| [3] |
Huang M, Cai S, Su J. The pathogenesis of sepsis and potential therapeutic targets[J]. Int J Mol Sci, 2019, 20(21): 5376.
doi: 10.3390/ijms20215376 URL |
| [4] |
Palmiere C, Augsburger M. Markers for sepsis diagnosis in the forensic setting: state of the art[J]. Croat Med J, 2014, 55(2): 103-114.
doi: 10.3325/cmj.2014.55.103 URL |
| [5] |
Francois B, Jeannet R, Daix T, et al. Interleukin-7 restores lymphocytes in septic shock: the IRIS-7 rando-mized clinical trial[J]. JCI Insight, 2018, 3(5): e98960.
doi: 10.1172/jci.insight.98960 URL |
| [6] |
Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3)[J]. JAMA, 2016, 315(8): 801-810.
doi: 10.1001/jama.2016.0287 URL |
| [7] |
Opal SM, Wittebole X. Biomarkers of infection and sepsis[J]. Crit Care Clin, 2020, 36(1): 11-22.
doi: 10.1016/j.ccc.2019.08.002 URL |
| [8] |
Pierrakos C, Velissaris D, Bisdorff M, et al. Biomarkers of sepsis: time for a reappraisal[J]. Crit Care, 2020, 24(1): 287.
doi: 10.1186/s13054-020-02993-5 URL |
| [9] |
Tang BM, Eslick GD, Craig JC, et al. Accuracy of procalcitonin for sepsis diagnosis in critically ill patients: systematic review and meta-analysis[J]. Lancet Infect Dis, 2007, 7(3): 210-217.
doi: 10.1016/S1473-3099(07)70052-X URL |
| [10] |
Tschaikowsky K, Hedwig-Geissing M, Schmidt J, et al. Lipopolysaccharide-binding protein for monitoring of postoperative sepsis: complemental to C-reactive protein or redundant?[J]. PLoS One, 2011, 6(8): e23615.
doi: 10.1371/journal.pone.0023615 URL |
| [11] | 路桂杰, 乐婷, 郭海云, 等. 白介素-6和降钙素原的动态变化对急诊老年脓毒性休克患者预后的评估意义[J]. 中国急救复苏与灾害医学杂志, 2017, 12(4): 321-323. |
| [12] |
Weidhase L, Wellhöfer D, Schulze G, et al. Is interleukin-6 a better predictor of successful antibiotic therapy than procalcitonin and C-reactive protein? A single center study in critically ill adults[J]. BMC Infect Dis, 2019, 19(1): 150.
doi: 10.1186/s12879-019-3800-2 pmid: 30760225 |
| [13] |
Jekarl DW, Lee SY, Lee J, et al. Procalcitonin as a diagnostic marker and IL-6 as a prognostic marker for sepsis[J]. Diagn Microbiol Infect Dis, 2013, 75(4): 342-347.
doi: 10.1016/j.diagmicrobio.2012.12.011 URL |
| [14] |
Thao PTN, Tra TT, Son NT, et al. Reduction in the IL-6 level at 24 h after admission to the intensive care unit is a survival predictor for Vietnamese patients with sepsis and septic shock: a prospective study[J]. BMC Emerg Med, 2018, 18(1): 39.
doi: 10.1186/s12873-018-0191-4 URL |
| [15] |
Song J, Park DW, Moon S, et al. Diagnostic and prognostic value of interleukin-6, pentraxin 3, and procalcitonin levels among sepsis and septic shock patients: a prospective controlled study according to the sepsis-3 definitions[J]. BMC Infect Dis, 2019, 19(1): 968.
doi: 10.1186/s12879-019-4618-7 URL |
| [16] |
Girardot T, Rimmelé T, Venet F, et al. Apoptosis-induced lymphopenia in sepsis and other severe injuries[J]. Apoptosis, 2017, 22(2): 295-305.
doi: 10.1007/s10495-016-1325-3 pmid: 27812767 |
| [17] |
Martin MD, Badovinac VP, Griffith TS. CD4 T cell responses and the sepsis-induced immunoparalysis state[J]. Front Immunol, 2020, 11: 1364.
doi: 10.3389/fimmu.2020.01364 URL |
| [18] |
Cabrera-Perez J, Condotta SA, Badovinac VP, et al. Impact of sepsis on CD4 T cell immunity[J]. J Leukoc Biol, 2014, 96(5): 767-777.
doi: 10.1189/jlb.5MR0114-067R URL |
| [19] |
Delano MJ, Ward PA. Sepsis-induced immune dysfunction: can immune therapies reduce mortality?[J]. J Clin Invest, 2016, 126(1): 23-31.
doi: 10.1172/JCI82224 URL |
| [20] | 蒋杰, 李鑫, 何发明, 等. 淋巴细胞减少在脓毒症患者预后评估中的应用价值[J]. 当代医学, 2019, 25(13): 7-10. |
| [21] | 赵群, 邹圣强, 章晋辉, 等. 老年脓毒症患者淋巴细胞水平的变化[J]. 中国老年学杂志, 2018, 15(38): 3704-3706. |
| [22] |
Chung KP, Chang HT, Lo SC, et al. Severe lymphopenia is associated with elevated plasma interleukin-15 levels and increased mortality during severe sepsis[J]. Shock, 2015, 43(6): 569-575.
doi: 10.1097/SHK.0000000000000347 URL |
| [1] | 周易, 陈影, 陈尔真. 甲状腺激素对脓毒症脏器功能维护作用的研究进展[J]. 内科理论与实践, 2022, 17(05): 408-412. |
| [2] | 郑毓真, 郑彦俊, 周易, 祁星, 陈薇薇, 史雯, 周伟君, 杨之涛, 陈影, 毛恩强, 陈尔真. 综合性医院674例脓毒症住院患者的回顾性临床分析[J]. 内科理论与实践, 2022, 17(04): 278-282. |
| [3] | 陈敏, 车在前, 陈影, 马丽, 赵冰, 周伟君, 毛恩强, 陈尔真. 白细胞血小板比值早期评估脓毒症预后的临床研究[J]. 内科理论与实践, 2022, 17(03): 208-213. |
| [4] | 李响, 王杨, 葛晓利, 潘曙明. 中药虎杖治疗脓毒症的研究进展[J]. 内科理论与实践, 2022, 17(01): 92-96. |
| [5] | 王雪洁, 陈孜瑾, 杜雯, 顾飞飞, 俞海瑾, 张文, 陈晓农. 不同病原菌致血流感染相关急性肾损伤的危险因素分析[J]. 内科理论与实践, 2021, 16(01): 22-26. |
| [6] | 方均燕, 宋阿会, 佟琰, 丁峰, 刘英莉. 脓毒症大鼠来源的外泌体对WJ-MSC的免疫调控能力的影响[J]. 组织工程与重建外科杂志, 2020, 16(3): 223-229. |
| [7] | 王秋云, 陈影, 赵冰, 孙思磊, 杨之涛, 毛恩强, 陈尔真. Sirt1通过HNF-1α/FXR-1通路调控脓毒症肝损伤的动物研究[J]. 诊断学理论与实践, 2020, 19(03): 279-285. |
| [8] | 李峰, 吴璟奕, 陈影, 陈尔真,. 普通肝素在治疗脓毒症中的应用[J]. 内科理论与实践, 2020, 15(01): 61-63. |
| [9] | 田芮, 刘嘉琳, 瞿洪平,. 脓毒症合并急性肾损伤患者血清血管生成素2、正五聚蛋白3水平的研究[J]. 内科理论与实践, 2019, 14(05): 313-316. |
| [10] | 赵婷, 陆运涛, 朱迎钢,. 长期住院高龄患者医院获得性肺炎病原学特点及早期炎症指标评估其预后的价值探讨[J]. 内科理论与实践, 2019, 14(04): 225-229. |
| [11] | 李艳秀, 左祥荣, 曹权,. 动态监测血小板计数对脓毒症患者预后评价的意义[J]. 内科理论与实践, 2018, 13(06): 354-357. |
| [12] | 李梅玲, 李磊, 张如愿, 刘嘉琳, 瞿洪平. 微量元素补充对术后脓毒症病人炎症反应的影响[J]. 外科理论与实践, 2018, 23(06): 533-538. |
| [13] | 宋剑峰, 陈尔真,. Apelin与脓毒症[J]. 内科理论与实践, 2017, 12(06): 416-418. |
| [14] | 张中文, 左祥荣, 李艳秀,. 降钙素原对外科脓毒症病人预后的判断价值[J]. 外科理论与实践, 2017, 22(05): 428-432. |
| [15] | 李艳秀, 左祥荣, 曹权,. 血小板计数水平对脓毒症患者的临床意义[J]. 内科理论与实践, 2017, 12(05): 351-354. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||