内科理论与实践 ›› 2022, Vol. 17 ›› Issue (04): 324-329.doi: 10.16138/j.1673-6087.2022.04.010
杨玲1, 查晴1, 张倩茹1, 叶佳雯1, 杨克2, 刘艳1( )
)
收稿日期:2021-12-10
出版日期:2022-07-18
发布日期:2022-08-08
通讯作者:
刘艳
E-mail:liuyan_ivy@126.com
基金资助:
YANG Ling1, ZHA Qing1, ZHANG Qianru1, YE Jiawen1, YANG Ke2, LIU Yan1()
Received:2021-12-10
Online:2022-07-18
Published:2022-08-08
Contact:
LIU Yan
E-mail:liuyan_ivy@126.com
摘要:
目的: 通过分析新的血清标志物与钙化性主动脉瓣膜病(calcific aortic valve disease,CAVD)关系,建立新的生物标志物预测模型,用于预测CAVD。方法: 收集446例心内科住院患者外周血及临床资料,通过SPSS20.0将患者按简单随机法分为筛查队列(n=202)和验证队列(n=244),酶联免疫吸附法检测胰高血糖素样肽1(glucagon-like peptide-1,GLP-1)和骨桥蛋白(osteopontin, OPN)血清浓度。通过分析筛查队列中各因子及临床变量与CAVD的关系,其后在验证队列中加以验证,构建CAVD预测模型。结果: 二元回归分析显示,筛查队列中多个因素与CAVD显著相关,最终确定高密度脂蛋白胆固醇(high density lipoprotein cholesterol,HDL-C)、GLP-1及OPN纳入预测模型,并绘制列线图。通过C统计量[筛查队列:0.73(95% 置信区间:0.66~0.80),验证队列0.70:(95% 置信区间:0.64~0.77)]及Hosmer-Lemeshow检验(筛查队列:P=0.14,验证队列:P=0.23)发现在筛查和验证队列中模型的区分度和一致性均表现良好。决策曲线分析显示,生物标志物模型比临床因素模型具有更高的净效益。此外,该模型在不同性别及年龄组仍具良好鉴别性。结论: GLP-1、OPN及HDL-C水平与CAVD具明显相关性。基于此,成功构建并验证了一种CAVD预测模型,该模型鉴别能力和准确性均表现良好,为预测CAVD提供可能。
中图分类号:
杨玲, 查晴, 张倩茹, 叶佳雯, 杨克, 刘艳. 钙化性主动脉瓣膜病的生物标志物预测模型的构建[J]. 内科理论与实践, 2022, 17(04): 324-329.
YANG Ling, ZHA Qing, ZHANG Qianru, YE Jiawen, YANG Ke, LIU Yan. Biomarker-based predictive model for calcific aortic valve disease[J]. Journal of Internal Medicine Concepts & Practice, 2022, 17(04): 324-329.
表1
筛查队列患者临床基本资料[$\bar{x}\pm s$/n(%)/M(Q1,Q3)]
| 变量 | β | SE | Wald χ2 | OR(95%CI) | P |
|---|---|---|---|---|---|
| 年龄 | 0.228 | 0.032 | 50.054 | 1.26(1.18~1.34) | 0.000 |
| 吸烟 | 1.099 | 0.490 | 5.038 | 3.00(1.15~7.84) | 0.025 |
| HDL-C | -1.551 | 0.674 | 5.290 | 0.21(0.06~0.80) | 0.021 |
| GLP-1 | -0.062 | 0.027 | 5.390 | 0.94(0.89~0.99) | 0.020 |
| OPN | 0.000 12 | 0.000 048 | 5.780 | 0.999 8(0.999 7~0.999 9) | 0.016 |
表2
验证队列患者临床基本资料[$\bar{x}\pm s$/n(%)/M(Q1,Q3)]
| 指标 | 非CAVD(n=99) | CAVD(n=103) | t/U/χ2 | P |
|---|---|---|---|---|
| 男性[n(%)] | 54(54.5) | 64(62.1) | 1.197 | 0.274 |
| 年龄(岁) | 60.19±8.24 | 73.44±7.65 | -11.845 | 0.000 |
| BMI(kg/m2) | 24(22,26) | 25(23,27) | -1.366 | 0.172 |
| 饮酒[n(%)] | 14(14.1) | 11(10.7) | 0.558 | 0.455 |
| 吸烟[n(%)] | 24(24.2) | 26(25.2) | 0.027 | 0.869 |
| GGT(U/L) | 19(13,35) | 21(16,28) | -0.819 | 0.413 |
| TG(mmol/L) | 1.48(1.15,2.10) | 1.43(1.02,2.14) | -0.612 | 0.541 |
| TC(mmol/L) | 4.04±1.13 | 4.02±1.22 | -0.119 | 0.906 |
| HDL-C(mmol/L) | 1.14(0.94,1.33) | 1.08(0.90,1.24) | -1.670 | 0.191 |
| LDL-C(mmol/L) | 2.34(1.72,2.77) | 2.42(1.76,2.92) | -0.479 | 0.584 |
| 空腹血糖(mmol/L) | 5.1(4.57,5.84) | 5.1(4.70,5.90) | -0.053 | 0.958 |
| BUN(mmol/L) | 5.0(4.2,5.7) | 5.6(4.5,6.7) | -2.647 | 0.008 |
| Cr(umol/L) | 73(63,84) | 82(71,97) | -4.162 | 0.000 |
| eGFR[mL/(min·1.73m2)] | 85.69±21.22 | 65.50±23.69 | 6.370 | 0.000 |
| 糖尿病[n(%)] | 35(35.4) | 33(32.0) | 0.248 | 0.618 |
| 高血压[n(%)] | 66(66.7) | 79(76.7) | 2.508 | 0.113 |
| CAD[n(%)] | 65(65.7) | 88(85.4) | 10.750 | 0.001 |
| 降糖药物治疗[n(%)] | 16(16.2) | 13(12.6) | 0.515 | 0.473 |
| 服用他汀类药物[n(%)] | 75(75.8) | 88(85.4) | 3.036 | 0.081 |
| GLP-1(ng/L) | 14.6(9.43,20.50) | 11.14(7.68,13.84) | -3.543 | 0.000 |
| OPN(ng/L) | 5 374.07(4 248.37,7 030.09) | 4 391.5(1 496.13,7 436.65) | -2.650 | 0.008 |
表3
二元Logistic回归分析各临床变量及生物标志物与CAVD间关系
| 指标 | 非CAVD(n=125) | CAVD(n=119) | t/U/χ2 | P |
|---|---|---|---|---|
| 男性[n(%)] | 69(55.2) | 71(59.7) | 0.497 | 0.481 |
| 年龄(岁) | 59.26±9.32 | 74.08±7.92 | -13.357 | 0.000 |
| BMI(kg/m2) | 24(23,27) | 25(23,28) | -1.090 | 0.276 |
| 饮酒[n(%)] | 15(12.0) | 7(5.9) | 2.781 | 0.095 |
| 吸烟[n(%)] | 42(33.6) | 27(22.7) | 3.578 | 0.059 |
| GGT(U/L) | 20(14,33) | 21(14,30) | -0.147 | 0.883 |
| TG(mmol/L) | 1.44(1.12,2.08) | 1.21(0.94,1.77) | -3.213 | 0.001 |
| TC(mmol/L) | 4.20±1.02 | 3.81±1.10 | 2.885 | 0.004 |
| HDL-C(mmol/L) | 1.09(0.92,1.29) | 1.04(0.91,1.19) | -1.992 | 0.046 |
| LDL-C(mmol/L) | 2.35(1.82,3.08) | 2.07(1.65,2.76) | -2.390 | 0.017 |
| 空腹血糖(mmol/L) | 4.82(4.49,5.59) | 4.94(4.55,5.86) | -0.682 | 0.495 |
| BUN(mmol/L) | 5.1(3.9,6.1) | 5.9(4.7,7.0) | -3.451 | 0.000 |
| Cr(μmol/L) | 72(62,85) | 82(69,96) | -3.967 | 0.000 |
| eGFR[mL/(min·1.73m2)] | 87.71±28.09 | 62.62±18.19 | 8.237 | 0.000 |
| 糖尿病[n(%)] | 40(32.0) | 33(27.7) | 0.530 | 0.467 |
| 高血压[n(%)] | 78(62.9) | 91(76.5) | 5.278 | 0.022 |
| CAD[n(%)] | 93(74.4) | 104(87.4) | 6.620 | 0.010 |
| 降糖药物治疗[n(%)] | 24(19.2) | 15(12.6) | 1.974 | 0.160 |
| 他汀类药物[n(%)] | 109(87.2) | 94(79.0) | 2.938 | 0.087 |
| GLP-1(ng/L) | 14.58(9.82,18.74) | 11.82(7.62,15.96) | -3.108 | 0.003 |
| OPN(ng/L) | 5 242.36(3 732.77,6799.75) | 3 941.64(1 469.97,7067.90) | -2.937 | 0.003 |
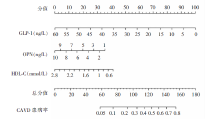
图1
基于生物标志物的CAVD预测模型
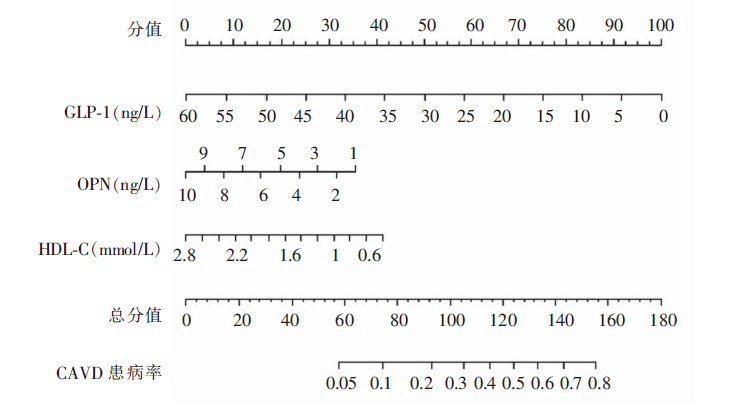
图2
生物标志物模型对CAVD的预测评估 A:筛查队列ROC曲线,AUC等于C统计量;B:验证队列ROC曲线,AUC等于C统计量;C:筛查队列校准曲线;D:验证队列校准曲线。
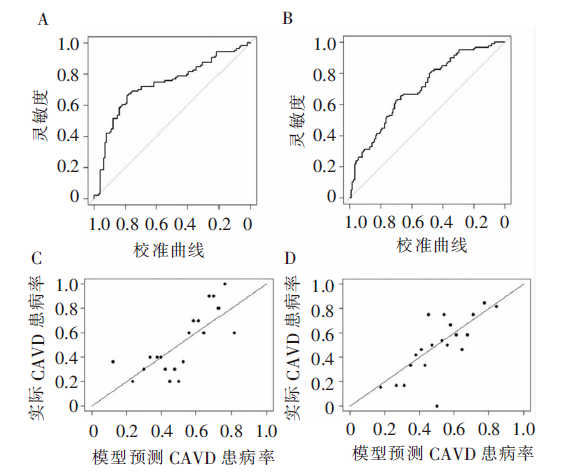
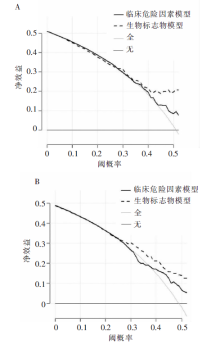
图3
生物标志物模型与临床危险因素模型DCA曲线 A:筛查队列;B:验证队列。
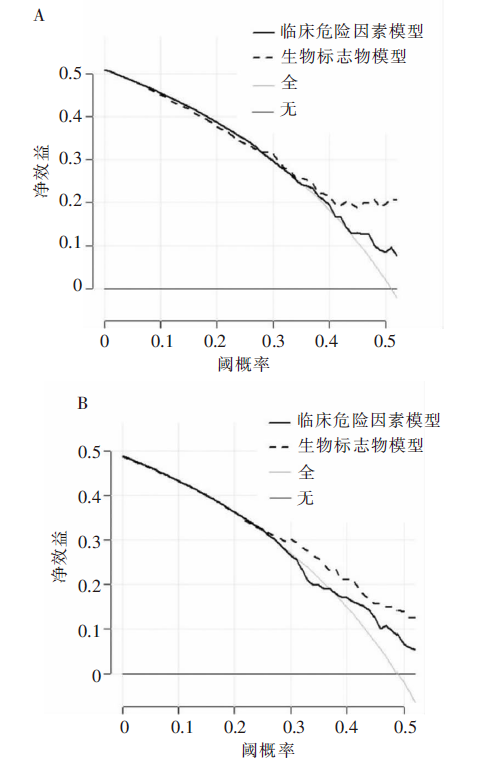
表4
在年龄、性别分层组中生物标志物模型预测CAVD表现
| 分组 | C统计量 | 95%CI |
|---|---|---|
| 男性组 | 0.79 | 0.70~0.88 |
| 女性组 | 0.64 | 0.52~0.76 |
| 青中年组(年龄<65岁) | 0.80 | 0.67~0.94 |
| 老年组(年龄≥65岁) | 0.73 | 0.65~0.81 |
| [1] |
Cho KI, Sakuma I, Sohn IS, et al. Inflammatory and metabolic mechanisms underlying the calcific aortic valve disease[J]. Atherosclerosis, 2018, 277: 60-65.
doi: 10.1016/j.atherosclerosis.2018.08.029 URL |
| [2] |
Alushi B, Curini L, Christopher MR, et al. Calcific aortic valve disease-natural history and future therapeutic strategies[J]. Front Pharmacol, 2020, 11: 685.
doi: 10.3389/fphar.2020.00685 URL |
| [3] |
Mathieu P, Arsenault BJ. CAVD: civilization aortic valve disease[J]. Eur Heart J, 2017, 38(28): 2198-2200.
doi: 10.1093/eurheartj/ehx219 URL |
| [4] | Yi B, Zeng W, Lv L, et al. Changing epidemiology of calcific aortic valve disease: 30-year trends of incidence, prevalence, and deaths across 204 countries and territories[J]. Aging (Albany NY), 2021, 13(9): 12710-12732. |
| [5] |
Coffey S, Cox B, Williams MJ. The prevalence, incidence, progression, and risks of aortic valve sclerosis: a systematic review and meta-analysis[J]. J Am Coll Cardiol, 2014, 63(25 Pt A): 2852-2861.
doi: 10.1016/j.jacc.2014.04.018 pmid: 24814496 |
| [6] |
Small A, Kiss D, Giri J, et al. Biomarkers of calcific aortic valve disease[J]. Arterioscler Thromb Vasc Bio, 2017, 37(4): 623-632.
doi: 10.1161/ATVBAHA.116.308615 URL |
| [7] |
Roumeliotis S, Roumeliotis A, Dounousi E, et al. Biomarkers of vascular calcification in serum[J]. Adv Clin Chem, 2020, 98: 91-147.
doi: S0065-2423(20)30016-0 pmid: 32564789 |
| [8] | Xiao F, Zha Q, Zhang Q, et al. Decreased glucagon-like peptide-1 is associated with calcific aortic valve disease: GLP-1 suppresses the calcification of aortic valve interstitial cells[J]. Front Cardiovasc Med, 2021, 8: 709741. |
| [9] | Chen Z, Chen L, Yao G, et al. Novel blood cytokine-based model for predicting severe acute kidney injury and poor outcomes after cardiac surgery[J]. J Am Heart Assoc, 2020, 9(22):e018004. |
| [10] |
Nie P, Yang G, Wang Z, et al. A CT-based radiomics nomogram for differentiation of renal angiomyolipoma without visible fat from homogeneous clear cell renal cell carcinoma[J]. Eur Radiol, 2020, 30(2): 1274-1284.
doi: 10.1007/s00330-019-06427-x URL |
| [11] |
Chen HY, Engert JC, Thanassoulis G. Risk factors for valvular calcification[J]. Curr Opin Endocrinol Diabetes Obes, 2019, 26(2): 96-102.
doi: 10.1097/MED.0000000000000471 pmid: 30694830 |
| [12] |
Vickers AJ, Elkin EB. Decision curve analysis: a novel method for evaluating prediction models[J]. Med Decis Making, 2006, 26: 565-574.
pmid: 17099194 |
| [13] | Summerhill VI, Moschetta D, Orekhov AN, et al. Sex-specific features of calcific aortic valve disease[J]. Int J Mol Sci, 2020, 21(16): 5620. |
| [14] |
Parolari A, Tremoli E, Cavallotti L, et al. Do statins improve outcomes and delay the progression of non-rheumatic calcific aortic stenosis?[J]. Heart, 2011, 97(7):523-529.
doi: 10.1136/hrt.2010.215046 URL |
| [15] |
Ardehali R, Leeper NJ, Wilson AM, et al. The effect of angiotensin-converting enzyme inhibitors and statins on the progression of aortic sclerosis and mortality[J]. J Heart Valve Dis, 2012, 21(3): 337-343.
pmid: 22808835 |
| [16] |
Choi B, Lee S, Kim SM, et al. Dipeptidyl peptidase-4 induces aortic valve calcification by inhibiting insulin-like growth factor-1 signaling in valvular interstitial cells[J]. Circulation, 2017, 135(20): 1935-1950.
doi: 10.1161/CIRCULATIONAHA.116.024270 URL |
| [17] |
Srivatsa SS, Harrity PJ, Maercklein PB, et al. Increased cellular expression of matrix proteins that regulate mineralization is associated with calcification of native human and porcine xenograft bioprosthetic heart valves[J]. J Clin Invest, 1997, 99(5): 996-1009.
pmid: 9062358 |
| [18] |
Sun JT, Chen YY, Mao JY, et al. Oxidized HDL, as a novel biomarker for calcific aortic valve disease, promotes the calcification of aortic valve interstitial cells[J]. J Cardiovasc Transl Res, 2019, 12(6): 560-568.
doi: 10.1007/s12265-019-09903-3 URL |
| [19] |
Myasoedova VA, Ravani AL, Frigerio B, et al. Novel pharmacological targets for calcific aortic valve disease: prevention and treatments[J]. Pharmacol Res, 2018, 136: 74-82.
doi: S1043-6618(18)31076-4 pmid: 30149054 |
| [20] |
Icer MA, Gezmen-Karadag M. The multiple functions and mechanisms of osteopontin[J]. Clin Biochem, 2018, 59: 17-24.
doi: 10.1016/j.clinbiochem.2018.07.003 URL |
| [1] | 段红燕, 唐国鑫, 盛捷, 曹孟杰, 裴磊, 田宏伟. 一种新型的疲劳强度预测模型[J]. 上海交通大学学报, 2022, 56(6): 801-808. |
| [2] | 闫晓红, 薄建萍. 呼出气一氧化氮在下气道慢性炎症疾病中的评估价值[J]. 内科理论与实践, 2022, 17(05): 418-422. |
| [3] | 周思锋, 徐海舒, 范欣生. 基于不同生物样本代谢组学的OSAHS生物标志物研究进展[J]. 诊断学理论与实践, 2022, 21(04): 535-540. |
| [4] | 蔡晓波, 王建香, 陆伦根. 胆汁淤积的生物标志物研究进展[J]. 内科理论与实践, 2022, 17(01): 11-14. |
| [5] | 祝颂, 钱晓超, 陆营波, 刘飞. 基于XGBoost的装备体系效能预测方法[J]. 空天防御, 2021, 4(2): 1-. |
| [6] | 肖凡, 查晴, 刘亚, 杨玲, 叶佳雯, 刘艳. 卵泡抑素样蛋白1对氧化低密度脂蛋白诱导血管平滑肌细胞增殖的影响[J]. 内科理论与实践, 2021, 16(03): 172-177. |
| [7] | 王泽田, 吴春荣, 齐越, 徐丹, 孙科远, 唐建国. 外泌体蛋白质组学分析白念珠菌感染小鼠的标志物[J]. 外科理论与实践, 2021, 26(03): 262-268. |
| [8] | 王佳琪, 马右维, 肖双涛, 黄雨达, 于志浩, 李征, 郑亚民. 胆囊胆固醇息肉与胆囊腺瘤的术前预测因素研究[J]. 外科理论与实践, 2021, 26(02): 144-148. |
| [9] | 赵春秀, 王晓龙. 呼出气分析在肺炎病原体诊断中的研究进展[J]. 内科理论与实践, 2021, 16(02): 138-140. |
| [10] | 李圳, 徐志红, 胡家安. 急性肺血栓栓塞症诊断相关生物标志物研究进展[J]. 内科理论与实践, 2021, 16(01): 60-63. |
| [11] | 张雪莹, 秦环龙. 肠道菌群作为结肠直肠癌生物标志物及其干预的临床意义[J]. 外科理论与实践, 2020, 25(02): 155-158. |
| [12] | 荣雪宁,卢浩,王明洋,文祝,戎晓力,王振. 基于刀盘扭转能量的土压平衡盾构刀具磨损分析[J]. 上海交通大学学报, 2019, 53(8): 965-970. |
| [13] | 李雪龙,于忠奇,赵亦希,EVSYUKOV S A. 多道次普旋预成形阶段法兰起皱预测[J]. 上海交通大学学报, 2019, 53(11): 1375-1380. |
| [14] | 陈海燕, 杨小宝, 许大康. 新生物标志物在胃肠道肿瘤中疗效预测和预后价值的研究进展[J]. 诊断学理论与实践, 2019, 18(06): 704-710. |
| [15] | 赵晴晴, 潘昱, 张一帆,. 胰高血糖素样肽1受体激动剂及二肽基肽酶4抑制剂在炎性疾病中的作用[J]. 内科理论与实践, 2019, 14(06): 381-385. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||