外科理论与实践 ›› 2022, Vol. 27 ›› Issue (05): 429-434.doi: 10.16139/j.1007-9610.2022.05.010
戴志强1,2, 郑金鑫1, 唐兆庆2, 张启2, 顾远2, 史忠义2, 胡国华1,2( ), 孙益红1,2()
), 孙益红1,2()
收稿日期:2022-04-21
出版日期:2022-09-25
发布日期:2022-11-10
通讯作者:
胡国华,孙益红
E-mail:sun.yihong@zs-hospital.sh.cn;hu.guohua@zs-hospital.sh.cn
基金资助:
DAI Zhiqiang1,2, ZHENG Jinxin1, TANG Zhaoqing2, ZHANG Qi2, GU Yuan2, SHI Zhongyi2, HU Guohua1,2(), SUN Yihong1,2()
Received:2022-04-21
Online:2022-09-25
Published:2022-11-10
Contact:
HU Guohua,SUN Yihong
E-mail:sun.yihong@zs-hospital.sh.cn;hu.guohua@zs-hospital.sh.cn
摘要: 目的 探讨胃癌病人淋巴结转移率分组界值及其对预后的评估。方法 回顾性分析2004年1月至2008年7月复旦大学附属中山医院392例行胃癌根治术,分期为美国癌症联合委员会(American Joint Committee on Cancer,AJCC)(第8版)Ⅱ~Ⅲ期的病人。利用X-tile软件进行淋巴结转移率的分组,评估淋巴结转移率与其他临床病理因素的相关性和对病人预后的评估。建立列线图预测模型,绘制校准曲线,与实际作比较。用Bootstrap法进行内部验证,计算一致性指数(C-index)评估模型准确性。结果 X-tile获得淋巴结转移率的最佳截断值为0.20(20%)和0.70(70%)。将淋巴结转移率分为1组(0~20%)、2组(21%~69%)和3组(70%~100%)。3组病人的生存差异有统计学意义(P<0.001)。单因素分析显示,淋巴结转移率、TNM分期、T分期、N分期、淋巴管浸润和年龄是影响预后的相关因素。多因素分析显示,淋巴结转移率、T分期、N分期、淋巴管浸润及年龄是影响预后的独立因素。分别以淋巴结转移率、TNM分期、淋巴管浸润及年龄绘制病人总体生存率的受试者操作特征曲线,其曲线下面积分别为0.699、0.667、0.587、0.561。采用淋巴结转移率、TNM分期、淋巴管浸润和年龄构建列线图预测模型,其C-index为0.707(95% CI:0.705~0.708)。校正曲线显示的1、3及5年预测生存率与实际相符。结论 淋巴结转移率是影响Ⅱ~Ⅲ期胃癌根治术后病人生存的独立危险因素。在判断Ⅱ~Ⅲ期胃癌根治术后病人预后时,淋巴结转移率是N分期的有效补充,可指导合理治疗。
中图分类号:
戴志强, 郑金鑫, 唐兆庆, 张启, 顾远, 史忠义, 胡国华, 孙益红. 淋巴结转移率对Ⅱ~Ⅲ期胃癌根治术后病人预后的评估[J]. 外科理论与实践, 2022, 27(05): 429-434.
DAI Zhiqiang, ZHENG Jinxin, TANG Zhaoqing, ZHANG Qi, GU Yuan, SHI Zhongyi, HU Guohua, SUN Yihong. Metastatic lymph node ratio to evaluate prognosis of patients with stage Ⅱ-Ⅲ gastric cancer after radical gastrectomy[J]. Journal of Surgery Concepts & Practice, 2022, 27(05): 429-434.
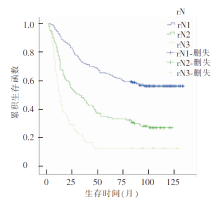
图1
不同rN亚组的总体生存曲线
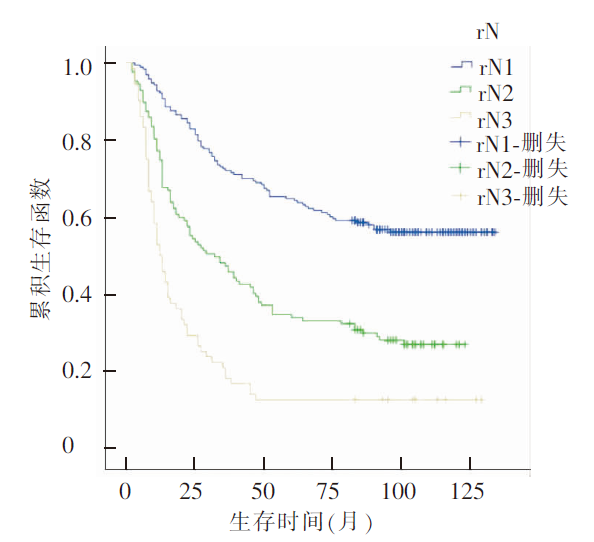
表1
病人rN与临床病理因素的关系[$\bar{x}±s$/n(%)]
| 临床病理因素 | 总体(n=392) | rN | 统计值 | P值 | ||
|---|---|---|---|---|---|---|
| rN1(n=193) | rN2(n=127) | rN3(n=72) | ||||
| 年龄(岁) | 61.3±11.6 | 61.8±11.3 | 60.5±11.5 | 61.6±12.4 | 0.473 | 0.624 |
| 性别[n(%)] | 2.149 | 0.341 | ||||
| 男 | 269(68.6) | 83(71.5) | 81(68.5) | 30(69.4) | ||
| 女 | 123(31.4) | 55(28.5) | 46(31.5) | 22(30.6) | ||
| 肿瘤部位[n(%)] | 11.331 | 0.023 | ||||
| 贲门 | 63(16.1) | 35(18.1) | 21(16.5) | 7(9.7) | ||
| 胃体 | 88(22.4) | 32(16.6) | 31(24.4) | 25(34.7) | ||
| 胃窦 | 241(61.5) | 126(65.3) | 75 (59.1) | 40(55.6) | ||
| 分化程度[n(%)] | 9.948 | 0.090 | ||||
| Ⅰ | 1(0.3) | 1(0.5) | 0(0) | 0(0) | ||
| Ⅱ | 70(17.9) | 45(23.3) | 18(14.2) | 7(9.7) | ||
| Ⅱ~Ⅲ | 25(6.4) | 12(6.2) | 9(7.1) | 4(5.6) | ||
| Ⅲ | 296(75.5) | 135(69.9) | 100(78.7) | 61(84.7) | ||
| T分期[n(%)] | 33.385 | <0.001 | ||||
| T1 | 8(2.0) | 1(0.5) | 6(4.7) | 1(1.4) | ||
| T2 | 28(7.1) | 19(9.8) | 8 (6.3) | 1(1.4) | ||
| T3 | 150(38.3) | 89(46.1) | 46(36.2) | 15(20.8) | ||
| T4 | 206(52.6) | 84(43.5) | 67(52.8) | 55(76.4) | ||
| N分期[n(%)] | 290.735 | <0.001 | ||||
| N0 | 60(15.5) | 56(33.2) | 3(2.4) | 1(1.4) | ||
| N1 | 73(18.5) | 73(40.1) | 0(0) | 0(0) | ||
| N2 | 92(23.4) | 59(27.2) | 32(25.2) | 1(1.4) | ||
| N3 | 167(27.2) | 5(1.1) | 92(72.4) | 70(97.2) | ||
| TNM分期[n(%)] | 107.082 | <0.001 | ||||
| Ⅱ | 115 (29.3) | 103(53.4) | 11(68.7) | 1(1.4) | ||
| Ⅲ | 277 (70.7) | 90(46.6) | 116(91.3) | 71(98.6) | ||
| 淋巴管浸润[n(%)] | 34.792 | <0.001 | ||||
| 有 | 98(25.0) | 23(11.9) | 47(37.0) | 28(38.9) | ||
| 无 | 294(75.0) | 170(88.1) | 80(63.0) | 44(61.1) | ||
| 神经侵犯[n(%)] | 2.215 | 0.344 | ||||
| 有 | 92(23.5) | 49(25.4) | 24(18.9) | 19(26.4) | ||
| 无 | 300(76.5) | 144(74.6) | 103(81.1) | 53(73.6) | ||
| 癌结节[n(%)] | 46.626 | 0.036 | ||||
| 有 | 67(17.1) | 35(18.1) | 14(11.0) | 18(25.0) | ||
| 无 | 325(82.9) | 158(81.9) | 113(89.0) | 54(75.0) | ||
表2
影响Ⅱ~Ⅲ期胃癌根治术后病人预后的单因素分析
| 临床病理因素 | β值 | 标准误 | Wald值 | 风险比 | 95%CI | P值 |
|---|---|---|---|---|---|---|
| 淋巴管浸润 | 0.693 | 0.139 | 24.747 | 2.000 | 1.522~2.629 | <0.001 |
| rN | 0.768 | 0.083 | 84.722 | 2.155 | 1.830~2.538 | <0.001 |
| 肿瘤部位 | -0.124 | 0.082 | 2.311 | 0.883 | 0.753~1.037 | 0.128 |
| 分化程度 | -0.084 | 0.079 | 1.137 | 0.919 | 0.787~1.073 | 0.286 |
| TNM分期 | 1.210 | 0.176 | 47.365 | 3.355 | 2.377~4.735 | <0.001 |
| T分期 | 0.347 | 0.098 | 12.466 | 1.414 | 1.167~1.715 | <0.001 |
| N分期 | 0.581 | 0.071 | 67.912 | 1.789 | 1.558~2.054 | <0.001 |
| 性别 | -0.049 | 0.138 | 0.124 | 0.952 | 0.727~0.248 | 0.724 |
| 癌结节 | 0.052 | 0.172 | 0.091 | 1.053 | 0.752~1.474 | 0.763 |
| 神经侵犯 | -0.044 | 0.154 | 0.083 | 0.957 | 0.708~1.293 | 0.774 |
| 年龄 | 0.298 | 0.131 | 5.214 | 1.347 | 1.043~1.740 | 0.022 |
表3
影响Ⅱ~Ⅲ期胃癌根治术后病人预后的多因素分析
| 临床病理因素 | β值 | 标准误 | Wald值 | 风险比 | 95%CI | P值 |
|---|---|---|---|---|---|---|
| 淋巴管浸润 | 0.322 | 0.146 | 4.851 | 1.380 | 1.036~1.838 | 0.028 |
| rN | 0.474 | 0.123 | 14.951 | 1.606 | 1.263~2.042 | <0.001 |
| T分期 | 0.200 | 0.093 | 4.661 | 1.222 | 1.019~1.466 | 0.031 |
| N分期 | 0.291 | 0.095 | 9.300 | 1.338 | 1.110~1.613 | 0.002 |
| 肿瘤部位 | -0.062 | 0.083 | 0.570 | 0.939 | 0.799~1.105 | 0.450 |
| 年龄 | 0.384 | 0.133 | 8.357 | 1.467 | 1.131~1.903 | 0.004 |
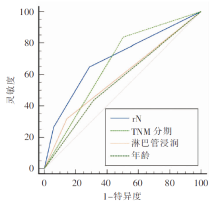
图2
以rN、TNM分期、淋巴管浸润及年龄绘制总体生存率ROC曲线
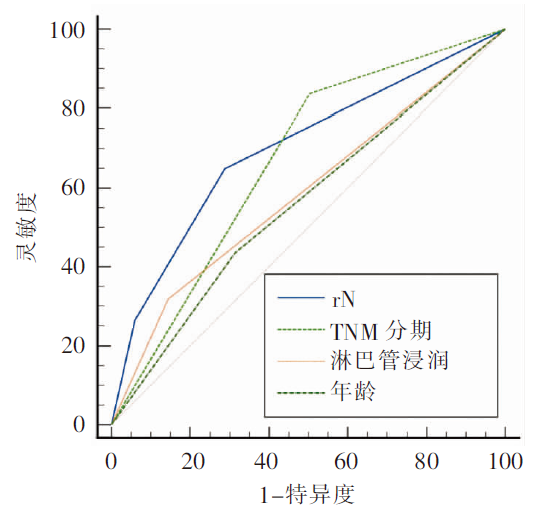
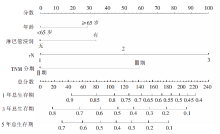
图3
Ⅱ~Ⅲ期胃癌病人根治术后预后的列线图
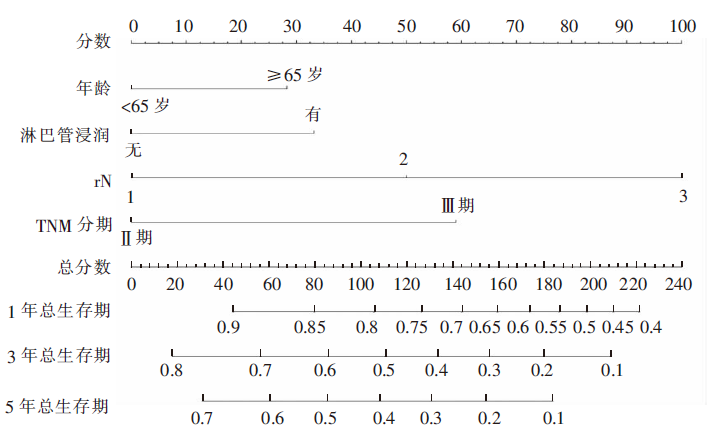
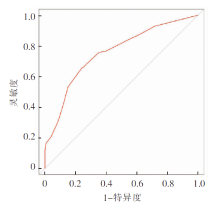
图4
列线图模型的评价
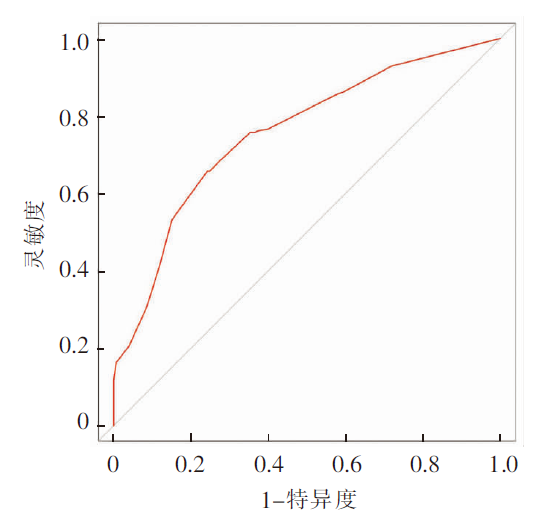
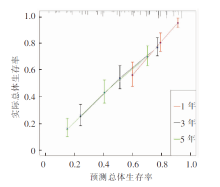
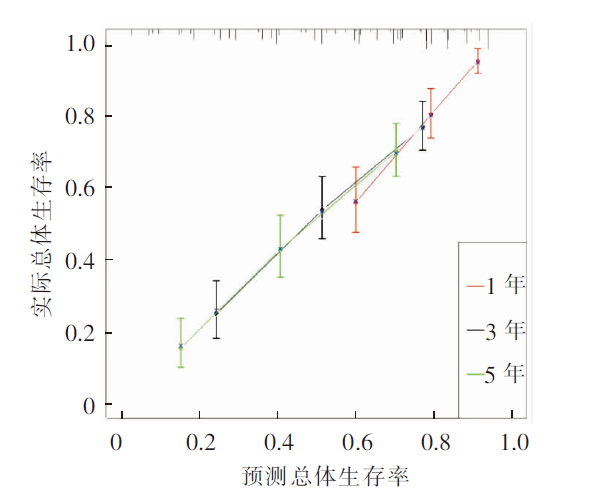
图5
1、3、5年生存率列线图模型校准曲线
| [1] | Biondi A, Persiani R, Cananzi F, et al. R0 resection in the treatment of gastric cancer: room for improvement[J]. World J Gastroenterol, 2010, 16(27):3358-3370. |
| [2] | 王鹏亮, 邓靖宇, 孙哲, 等. pN3b期胃癌亚分期预后评估的合理性研究[J]. 中国肿瘤临床, 2021, 48(3):118-124. |
| [3] | 季加孚, 陕飞. 中国胃癌外科发展的机遇与挑战[J]. 中华消化外科杂志, 2018, 17(1):18-21. |
| [4] | Ajani JA, D′Amico TA, Almhanna K, et al. Gastric cancer, version 3.2016, NCCN clinical practice guidelines in oncology[J]. J Natl Compr Canc Netw, 2016, 14(10):1286-1312. |
| [5] | 朱志, 杜雨薇, 刘福囝, 等. 淋巴结转移在胃癌预后中的评价[J]. 腹部外科, 2021, 34(3):179-183,188. |
| [6] | Kano K, Yamada T, Oshima T. ASO author reflections: association between the lymph node ratio and survival in patients with pathological stage Ⅱ/Ⅲ gastric cancer[J]. Ann Surg Oncol, 2020, 27(11):4248-4249. |
| [7] | 梁寒. 胃癌手术治疗已进入精细化管理时代: 解读第5版日本胃癌治疗指南和第15版日本胃癌处理规约[J]. 中华肿瘤杂志, 2019, 41(3):168-172. |
| [8] | Zhu Y, Fang X, Wang L, et al. Predictive nomogram for early death of metastatic gastric cancer: a retrospective study in the SEER database and China[J]. J Cancer, 2020, 11(18):5527-5535. |
| [9] | Amin MB, Greene FL, Edge SB, et al. The Eighth Edition AJCC Cancer Staging Manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging[J]. CA Cancer J Clin, 2017, 67(2):93-99. |
| [10] | 潘源, 梁寒, 薛强, 等. 国际抗癌联盟和日本胃癌协会胃癌淋巴结分期法与国人胃癌患者预后相关性的比较[J]. 中华肿瘤杂志, 2008, 30(5):376-380. |
| [11] | Kodera Y, Yamamura Y, Shimizu Y, et al. Lymph node status assessment for gastric carcinoma: is the number of metastatic lymph nodes really practical as a parameter for N categories in the TNM Classification? tumor node metastasis[J]. J Surg Oncol, 1998, 69(1):15-20. |
| [12] | Kutlu OC, Watchell M, Dissanaike S. Metastatic lymph node ratio successfully predicts prognosis in western gastric cancer patients[J]. Surg Oncol, 2015, 24(2):84-88. |
| [13] | Wang J, Dang P, Raut CP, et al. Comparison of a lymph node ratio-based staging system with the 7th AJCC system for gastric cancer: analysis of 18,043 patients from the SEER database[J]. Ann Surg, 2012, 255(3):478-485. |
| [14] | Saito H, Fukumoto Y, Osaki T, et al. Prognostic significance of the ratio between metastatic and dissected lymph nodes (n ratio) in patients with advanced gastric cancer?[J]. J Surg Oncol, 2008, 97(2):132-135. |
| [15] | Wu L, Liang Y, Zhang C, et al. Prognostic significance of lymphovascular infiltration in overall survival of gastric cancer patients after surgery with curative intent[J]. Chin J Cancer Res, 2019, 31(5):785-796. |
| [16] | International Bladder Cancer Nomogram Consortium, Bochner BH, Kattan MW, et al. Postoperative nomogram predicting risk of recurrence after radical cystectomy for bladder cancer[J]. J Clin Oncol, 2006, 24(24):3967-3972. |
| [17] | Li Y, Jia H, Yu W, et al. Nomograms for predicting prognostic value of inflammatory biomarkers in colorectal cancer patients after radical resection[J]. Int J Cancer, 2016, 139(1):220-231. |
| [1] | 严超, 陆晟, 燕敏, 朱正纲. 《日本胃癌治疗指南2021(第6版)》解读及瑞金实践[J]. 外科理论与实践, 2023, 28(04): 326-354. |
| [2] | 孙祺, 黄文博, 何炳良, 刘畅, 徐宇航, 赵伟. 预防性腹腔热灌注化疗对局部进展期胃癌根治术后病人预后改善的有效性研究[J]. 外科理论与实践, 2023, 28(04): 366-370. |
| [3] | 孙强, 姚骏, 张鑫, 杜杉珊, 王伟军. 近端胃切除抗反流消化道重建方式的研究进展[J]. 外科理论与实践, 2023, 28(04): 388-393. |
| [4] | 胡文庆, 杨垠浩, 崔鹏, 魏伟. 食管胃结合部腺癌腹腔镜经腹-左膈肌路径近端胃加食管下段切除高位消化道重建现状[J]. 外科理论与实践, 2023, 28(03): 226-232. |
| [5] | 燕速, 郑民华. 中国单孔及减孔腹腔镜胃癌手术实践[J]. 外科理论与实践, 2023, 28(03): 233-239. |
| [6] | 范清泉, 宋晓玲, 顾钧. 外泌体在胃癌中的研究展望[J]. 外科理论与实践, 2023, 28(02): 177-180. |
| [7] | 徐凯, 李百文. 早期胃癌及胃癌前病变的内镜黏膜下剥离术治疗[J]. 内科理论与实践, 2023, 18(02): 102-106. |
| [8] | 颜凌, 王凌云, 陈勇, 杜联军. 双能CT图像深度学习重建算法在胃癌术前T分期中的应用[J]. 诊断学理论与实践, 2023, 22(02): 154-159. |
| [9] | 李建芳, 余俊贤, 严超, 朱正纲, 刘炳亚. 胃癌基础与转化研究的热点问题[J]. 外科理论与实践, 2023, 28(01): 7-16. |
| [10] | 卢一鸣, 熊建平, 田艳涛. 晚期胃癌转化治疗的发展现状与研究前景[J]. 外科理论与实践, 2023, 28(01): 17-23. |
| [11] | 胡端敏. 内镜超声检查对胃癌浸润深度的判断及影响因素[J]. 诊断学理论与实践, 2023, 22(01): 85-88. |
| [12] | 朱正纲. 胃癌外科综合治疗的若干进展与展望[J]. 外科理论与实践, 2023, 28(01): 1-6. |
| [13] | 赵法之, 赵平. 胃癌治疗手术中心论体系的形成与完善[J]. 外科理论与实践, 2023, 28(01): 24-30. |
| [14] | 李国立, 郭飞龙. 动静脉结合术前化疗在进展期胃癌治疗中的应用[J]. 外科理论与实践, 2023, 28(01): 31-35. |
| [15] | 刘文韬, 刘福坤. 中国胃癌围术期综合治疗概述与展望[J]. 外科理论与实践, 2023, 28(01): 36-41. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||