外科理论与实践 ›› 2023, Vol. 28 ›› Issue (06): 529-535.doi: 10.16139/j.1007-9610.2023.06.08
蔡晓雨1, 张瑞国2, 胡玉敬1, 王任飞3( ), 边艳珠1()
), 边艳珠1()
收稿日期:2023-09-26
出版日期:2023-11-25
发布日期:2024-03-04
通讯作者:
边艳珠,E-mail:yanzhubian99@163.com;王任飞,E-mail: roslyn_en@163.com
CAI Xiaoyu1, ZHANG Ruiguo2, HU Yujing1, WANG Renfei3(), BIAN Yanzhu1()
Received:2023-09-26
Online:2023-11-25
Published:2024-03-04
摘要:
目的: 分析术后接受131I治疗的乳头状甲状腺微小癌(papillary thyroid microcarcinoma, PTMC)与乳头状甲状腺非微小癌(papillary thyroid non-microcarcinoma, non-PTMC)病人的临床病理特征,并比较治疗转归的差异,以期指导PTMC的131I治疗决策。方法: 纳入2015年1月至2020年12月在天津医科大学总医院核医学科131I治疗的1 118例PTC病人,采用卡方检验及秩和检验比较PTMC组与non-PTMC组病人临床病理特征、131I治疗情况及治疗反应的差异,Kaplan-Meier法绘制两组的治疗反应不佳(incomplete response, IR)率曲线。结果: PTMC组病人多灶性、累及双叶的比例均高于non-PTMC组,腺外侵犯、T4、N1b、刺激性甲状腺球蛋白(stimulated thyroglobulin, sTg)>10 μg/L及高危复发风险的比例低于non-PTMC组(P<0.05)。PTMC组多数病人首次接受清甲治疗,而non-PTMC组中更多病人接受辅助及清灶治疗(P<0.05)。两组病人131I治疗反应、疗效满意(excellent response, ER)率和IR率的差异均无统计学意义,IR率曲线差异也无统计学意义(P>0.05)。结论: PTMC具有一定的侵袭性。经综合评估和规范131I治疗后,PTMC和non-PTMC病人治疗转归大致相同。PTMC的界定对131I治疗决策的指导价值极其有限。
中图分类号:
蔡晓雨, 张瑞国, 胡玉敬, 王任飞, 边艳珠. 乳头状甲状腺微小癌不宜作为术后131I治疗的决策依据[J]. 外科理论与实践, 2023, 28(06): 529-535.
CAI Xiaoyu, ZHANG Ruiguo, HU Yujing, WANG Renfei, BIAN Yanzhu. Papillary thyroid microcarcinoma should not be used as the basis for postoperative 131I therapy[J]. Journal of Surgery Concepts & Practice, 2023, 28(06): 529-535.
表1
PTMC与non-PTMC病人临床病理特征比较[n(%)]
| Characteristics | PTMC(n=458) | non-PTMC(n=660) | Test value | P value | |
|---|---|---|---|---|---|
| Age(year) | <55 | 359(78.4) | 507(76.8) | 0.380 | 0.561 |
| ≥55 | 99(21.6) | 153(23.2) | |||
| Gender | Male | 130(28.4) | 223(33.8) | 3.654 | 0.058 |
| Female | 328(71.6) | 437(66.2) | |||
| Number of lesions | Unifocal | 132(28.8) | 263(39.8) | 14.390 | 0.000 |
| Multifocal | 326(71.2) | 397(60.2) | |||
| Involvement of thyroid lobes | Unilateral thyroid lobe | 193(42.1) | 325(49.2) | 5.485 | 0.021 |
| Bilateral thyroid lobes | 265(57.9) | 335(50.8) | |||
| Pathological subtype | Non-invasive | 451(98.5) | 642(97.3) | 1.778 | 0.220 |
| Invasive | 7(1.5) | 8(2.7) | |||
| Extra-thyroid extension | No | 350(76.4) | 413(62.6) | 23.910 | 0.000 |
| Yes | 108(23.6) | 247(37.4) | |||
| T4 stage | No | 431(94.1) | 593(89.8) | 6.361 | 0.012 |
| Yes | 27(5.9) | 67(10.2) | |||
| lymph node metastasis | N0 | 91(19.9) | 102(15.5) | 23.382 | 0.000 |
| N1a | 224(48.9) | 257(38.9) | |||
| N1b | 143(31.2) | 301(45.6) | |||
| Distant metastasis | No | 441(96.3) | 625(94.7) | 1.544 | 0.249 |
| Yes | 17(3.7) | 35(5.3) | |||
| sTg of pre-therapy(μg/L) | <1 | 162(35.4) | 158(23.9) | 24.321 | 0.000 |
| 1-10 | 209(45.6) | 307(46.5) | |||
| ≥10 | 87(19.0) | 195(29.5) | |||
| Recurrence risk stratification | Low risk | 65(14.2) | 50(7.6) | 30.800 | 0.000 |
| Moderate risk | 272(59.4) | 340(51.5) | |||
| High risk | 121(26.4) | 270(40.9) | |||
表2
PTMC与non-PTMC病人接受131I治疗情况比较[n(%)]
| Item | PTMC(n=458) | non-PTMC(n=660) | Test value | P value | |
|---|---|---|---|---|---|
| Goal of the initial therapy | Remnant ablation | 294(64.2) | 308(46.7) | 34.492 | 0.000 |
| Adjuvant therapy | 138(30.1) | 282(42.7) | |||
| 131I therapy | 26(5.7) | 70(10.6) | |||
| Initial therapeutic doses(GBq) | ≤3.7 | 294(64.2) | 308(46.7) | 34.492 | 0.000 |
| 5.55 | 138(30.1) | 282(42.7) | |||
| 7.4 | 26(5.7) | 70(10.6) | |||
| Cumulative therapeutic doses(GBq) | ≤7.4 | 383(83.6) | 465(70.5) | 26.724 | 0.000 |
| 7.4-22.2 | 72(15.7) | 190(28.8) | |||
| >22.2 | 3(0.7) | 5(0.8) | |||
| Times of 131I therapy | Single | 352(76.9) | 417(63.2) | 23.545 | 0.000 |
| Multiple | 106(23.1) | 243(36.8) | |||
表3
接受清甲治疗的PTMC与non-PTMC病人治疗反应比较[n(%)]
| Item | 6 months after 131I therapy | Last follow-up | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| PTMC(n=458) | non-PTMC(n=660) | Test value | P value | PTMC(n=458) | non-PTMC(n=660) | Test value | P valu | |||
| Therapeutic response | ER | 189(64.3) | 178(57.8) | 4.911 | 0.189 | 220(74.8) | 235(76.3) | 4.662 | 0.147 | |
| IDR | 103(35.0) | 122(39.6) | 74(25.2) | 68(22.1) | ||||||
| BIR | 1(0.3) | 4(1.3) | 0 | 3(1.0) | ||||||
| SIR | 1(0.3) | 4(1.3) | 0 | 2(0.6) | ||||||
| ER | ER | 189(64.3) | 178(57.8) | 2.665 | 0.113 | 220(74.8) | 235(76.3) | 0.176 | 0.705 | |
| Non-ER | 105(35.7) | 130(42.2) | 74(25.2) | 73(23.7) | ||||||
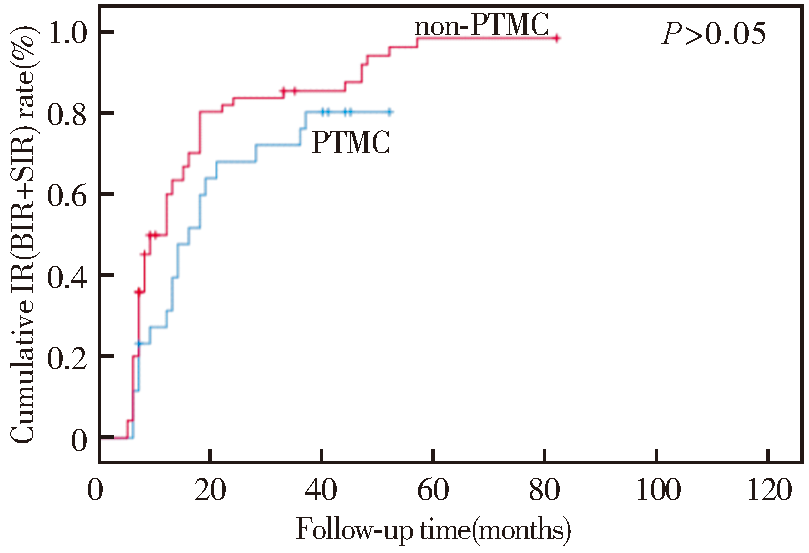
| IR | IR | 2(0.7) | 8(2.6) | 2.312 | 0.128 | 0 | 5(1.6) | — | 0.062 | |
| Non-IR | 292(99.3) | 300(97.4) | 294(100.0) | 303(98.4) | ||||||
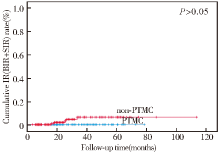
图1
接受清甲治疗的PTMC与non-PTMC病人IR率图
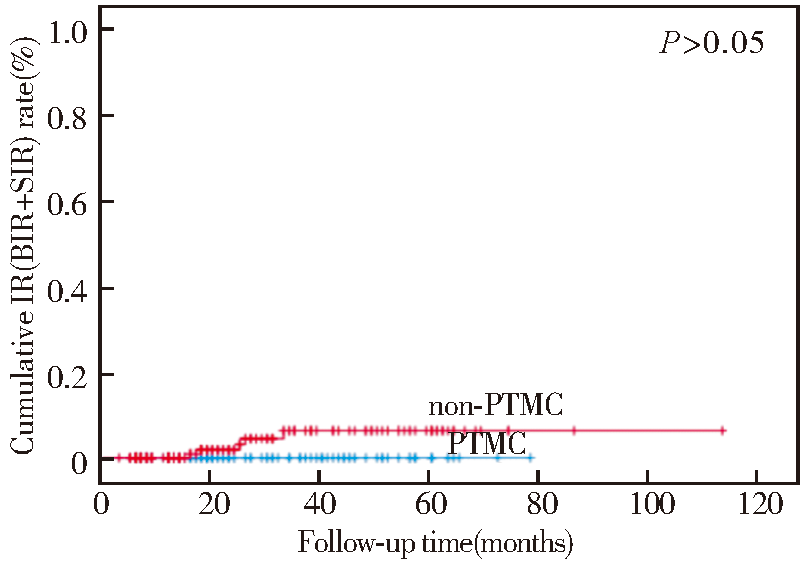
表4
接受辅助治疗的PTMC与non-PTMC病人治疗反应比较[n(%)]
| Item | 6 months after 131I therapy | Last follow-up | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| PTMC(n=458) | non-PTMC(n=660) | Test value | P value | PTMC(n=458) | non-PTMC(n=660) | Test value | P value | |||
| Therapeutic response | ER | 53(38.4) | 86(30.5) | 4.950 | 0.173 | 71(51.4) | 133(47.2) | 1.978 | 0.575 | |
| IDR | 37(26.8) | 85(30.1) | 41(29.7) | 88(31.2) | ||||||
| BIR | 32(23.3) | 87(30.9) | 17(12.3) | 47(16.7) | ||||||
| SIR | 16(11.6) | 24(8.5) | 9(6.5) | 14(5.0) | ||||||
| ER | ER | 53(38.4) | 86(30.5) | 2.618 | 0.122 | 71(51.4) | 133(47.2) | 0.681 | 0.467 | |
| Non-ER | 85(61.6) | 196(69.5) | 67(48.6) | 149(52.8) | ||||||
| IR | IR | 48(34.8) | 111(39.4) | 0.862 | 0.393 | 26(18.8) | 61(21.6) | 0.439 | 0.525 | |
| Non-IR | 90(65.2) | 171(60.6) | 112(81.2) | 221(78.4) | ||||||
| SIR | SIR | 16(11.6) | 24(8.5) | 1.022 | 0.376 | 9(6.5) | 14(5.0) | 0.434 | 0.649 | |
| Non-SIR | 122(88.4) | 258(91.5) | 129(93.5) | 268(95.0) | ||||||
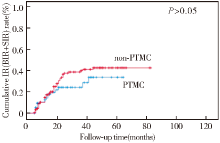
图2
接受辅助治疗的PTMC与non-PTMC病人IR率图
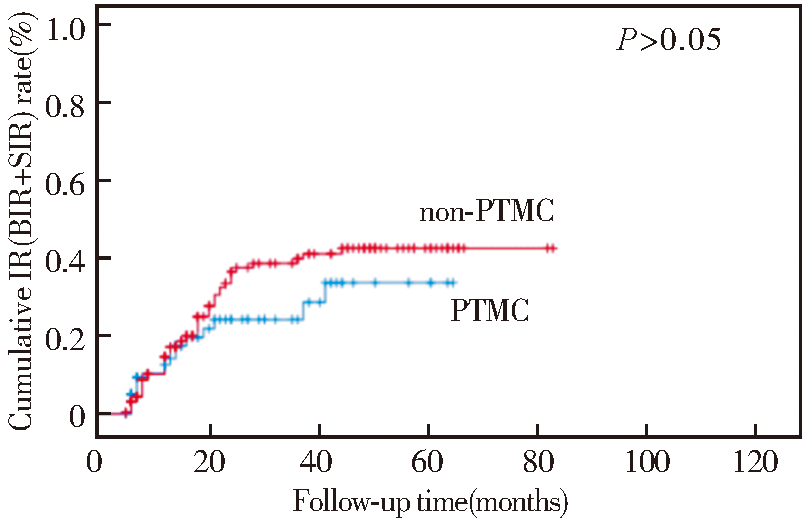
表5
接受清灶治疗的PTMC与non-PTMC病人末次随访治疗反应比较[n(%)]
| Item | PTMC (n=458) | non-PTMC (n=660) | Test value | P value | |
|---|---|---|---|---|---|
| Therapeutic response | ER | 1(3.8) | 3(4.3) | 1.693 | 0.685 |
| IDR | 2(7.7) | 6(8.6) | |||
| BIR | 4(15.4) | 19(27.1) | |||
| SIR | 19(73.1) | 42(60.0) | |||
| ER | ER | 1(3.8) | 3(4.3) | — | 1.000 |
| Non-ER | 25(96.2) | 67(95.7) | |||
| IR | IR | 23(88.5) | 61(87.1) | 0.000 | 1.000 |
| Non-IR | 3(11.5) | 9(12.9) | |||
| SIR | SIR | 19(73.1) | 42(60.0) | 1.399 | 0.340 |
| Non-SIR | 7(26.9) | 28(40.0) | |||
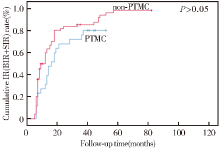
图3
接受清灶治疗的PTMC与non-PTMC病人IR率图
| [1] | HEDINGER C. Histological typing of thyroid tumours[J]. WHO, 1988,11. |
| [2] |
TUTTLE R M, HADDAD R I, BALL D W, et al. Thyroid carcinoma, version 2.2014[J]. J Natl Compr Canc Netw, 2014, 12(12):1671-1680.
doi: 10.6004/jnccn.2014.0169 URL |
| [3] |
CHOW S M, LAW S C, CHAN J K, et al. Papillary microcarcinoma of the thyroid-prognostic significance of lymph node metastasis and multifocality[J]. Cancer, 2003, 98(1):31-40.
doi: 10.1002/cncr.v98:1 URL |
| [4] |
HAY I D. Management of patients with low-risk papillary thyroid carcinoma-sciencedirect[J]. Endocr Pract, 2007, 13(5):521-533.
doi: 10.4158/EP.13.5.521 pmid: 17872355 |
| [5] |
NAM-GOONG I S, KIM H Y, GONG G, et al. Ultrasonography-guided fine-needle aspiration of thyroid incidentaloma:correlation with pathological findings[J]. Clin Endocrinol(Oxf), 2004, 60(1):21-28.
doi: 10.1046/j.1365-2265.2003.01912.x URL |
| [6] |
DAVIES L, WELCH H G. Current thyroid cancer trends in the United States[J]. JAMA Otolaryngol Head Neck Surg, 2014, 140(4):317-322.
doi: 10.1001/jamaoto.2014.1 URL |
| [7] |
HAY I D, HUTCHINSON M E, GONZALEZ-LOSADA T, et al. Papillary thyroid microcarcinoma: a study of 900 cases observed in a 60-year period[J]. Surgery, 2008, 144(6):980-987;discussion 987-988.
doi: 10.1016/j.surg.2008.08.035 URL |
| [8] |
WANG T S, GOFFREDO P, SOSA J A, et al. Papillary thyroid microcarcinoma:an over-treated malignancy?[J]. World J Surg, 2014, 38(9):2297-2303.
doi: 10.1007/s00268-014-2602-3 URL |
| [9] |
CAPPELLI C, CASTELLANO M, BRAGA M, et al. Aggressiveness and outcome of papillary thyroid carcinoma (PTC) versus microcarcinoma (PMC): a mono-institutional experience[J]. J Surg Oncol, 2007, 95(7):555-560.
doi: 10.1002/jso.v95:7 URL |
| [10] |
XUE S, WANG P, LIU J, et al. Radioactive Iodine ablation decrease recurrences in papillary thyroid microcarcinoma with lateral lymph node metastasis in Chinese patients[J]. World J Surg, 2017, 41(12):3139-3146.
doi: 10.1007/s00268-017-4134-0 pmid: 28741199 |
| [11] |
YANG T, ZHENG S Y, JIAO J, et al. Radioiodine remnant ablation in papillary thyroid microcarcinoma: a meta-analysis[J]. Nucl Med Commun, 2019, 40(7):711-719.
doi: 10.1097/MNM.0000000000001018 pmid: 31095043 |
| [12] | PELLEGRITI G, FRASCA F, REGALBUTO C, et al. Worldwide increasing incidence of thyroid cancer: update on epidemiology and risk factors[J]. J Cancer Epidemiol, 2013, 2013:965212. |
| [13] |
PAPINI E, GUGLIELMI R, GHARIB H, et al. Ultrasound-guided laser ablation of incidental papillary thyroid microcarcinoma: a potential therapeutic approach in patients at surgical risk[J]. Thyroid, 2011, 21(8):917-920.
doi: 10.1089/thy.2010.0447 pmid: 21595556 |
| [14] | 冯思源, 郑薇, 张瑞国, 等. 甲状腺微小乳头状癌与乳头状非微小癌的临床特点及131I疗效的比较研究[J]. 国际放射医学核医学杂志, 2018, 42(2):111-114. |
| FENG S Y, ZHENG W, ZHANG R G, et al. Clinical cha-racteristics and131I efficacy of papillary thyroid microcarcinoma and papillary thyroid non-micro carcinoma[J]. Int J Radiat Med Nucl Med, 2018, 42(2):111-114. | |
| [15] |
KWAK J Y, KIM E K, KIM M J, et al. Papillary microcarcinoma of the thyroid: predicting factors of lateral neck node metastasis[J]. Ann Surg Oncol, 2009, 16(5):1348-1355.
doi: 10.1245/s10434-009-0384-x pmid: 19224278 |
| [16] |
ZHENG W, WANG K, WU J, et al. Multifocality is associated with central neck lymph node metastases in papillary thyroid microcarcinoma[J]. Cancer Manag Res, 2018, 10:1527-1533.
doi: 10.2147/CMAR.S163263 pmid: 29942154 |
| [17] |
LUO Y, ZHAO Y, CHEN K, et al. Clinical analysis of cervical lymph node metastasis risk factors in patients with papillary thyroid microcarcinoma[J]. J Endocrinol Invest, 2019, 42(2):227-236.
doi: 10.1007/s40618-018-0908-y pmid: 29876836 |
| [18] |
OZER B, SIT M, AKTAS G, et al. Detection rate of thyroid papillary micro-carcinoma in multinodular goiter surgery[J]. J Coll Physicians Surg Pak, 2019, 29(4):353-355.
doi: 10.29271/jcpsp.2019.04.353 pmid: 30925960 |
| [19] |
GU J H, ZHAO Y N, XIE R L, et al. Analysis of risk factors for cervical lymph node metastasis of papillary thyroid microcarcinoma: a study of 268 patients[J]. BMC Endocr Disord, 2019, 19(1):124.
doi: 10.1186/s12902-019-0450-8 |
| [20] |
ZHENG X, PENG C, GAO M, et al. Risk factors for cervical lymph node metastasis in papillary thyroid microcarcinoma: a study of 1,587 patients[J]. Cancer Biol Med, 2019, 16(1):121-130.
doi: 10.20892/j.issn.2095-3941.2018.0125 pmid: 31119052 |
| [21] | 中国抗癌协会甲状腺癌专业委员会CATO. 甲状腺微小乳头状癌诊断与治疗中国专家共识(2016版)[J]. 中国肿瘤临床, 2016, 43(10):405-411. |
| Chinese Association of Thyroid Oncology. Chinese expert consensus on the diagnosis and treatment of micropapillary thyroid cancer (2016 Edition)[J]. Chin J Clin Oncol, 2016, 43(10):405-411. | |
| [22] |
KIM H Y, PARK W Y, LEE K E, et al. Comparative analysis of gene expression profiles of papillary thyroid microcarcinoma and papillary thyroid carcinoma[J]. J Cancer Res Ther, 2010, 6(4):452-457.
doi: 10.4103/0973-1482.77103 pmid: 21358079 |
| [23] |
HAUGEN B R, ALEXANDER E K, BIBLE K C, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer[J]. Thyroid, 2016, 26(1):1-133.
doi: 10.1089/thy.2015.0020 URL |
| [24] | 中国临床肿瘤学会甲状腺癌专业委员会, 中国研究型医院学会分子诊断专业委员会甲状腺癌学组, 医促会甲状腺疾病专业委员会核医学组, 等. 分化型甲状腺癌术后131I治疗前评估专家共识[J]. 中国癌症杂志, 2019, 29(10):832-840. |
| Thyroid Cancer Committee of Chinese Society of Clinical Oncology, Thyroid Cancer Group of Molecular Diagnosis Committee of Chinese Society of Research Hospitals, Nuclear Medicine Group of Thyroid Disease Committee of Association for the Promotion of Medical Science, et al. Expert consensus on pre-treatment evaluation of postoperative 131I therapy for differentiated thyroid cancer[J]. China Oncol, 2019, 29(10):832-840. |
| [1] | 武晓莉 班耀林 陈立彬 谢春晖 马倩玉 王文波.
“核心剥离式”瘢痕疙瘩修薄术联合放疗的疗效分析
[J]. 组织工程与重建外科杂志, 2023, 19(1): 22-. |
| [2] | 汤玲琳, 李莉, 来益, 刘建军, 周翔. 中危甲状腺乳头状癌病人131I治疗后肿瘤复发因素分析[J]. 外科理论与实践, 2023, 28(06): 536-539. |
| [3] | 廖振宇, 赵起悟, 匡洁, 刘卓然, 孙寒星, 王越, 邱伟华, 陈曦, 严佶祺. 高细胞亚型甲状腺乳头状癌的侵袭性组织病理学特征研究[J]. 外科理论与实践, 2023, 28(06): 524-528. |
| [4] | 江弘毅, 郑传铭, 葛明华. 甲状腺肿瘤微创外科进展[J]. 外科理论与实践, 2023, 28(06): 491-495. |
| [5] | 贺文, 顾建华, 邢戌健, 翁子毅, 费健. 术中发现气管憩室2例病例报告并文献复习[J]. 外科理论与实践, 2023, 28(04): 383-387. |
| [6] | 孔韦奇, 何俊, 杨成广, 刘微薇, 徐英杰. 嗜铬细胞瘤合并甲状腺乳头状癌(附1例报告)[J]. 外科理论与实践, 2023, 28(02): 162-165. |
| [7] | 颜海波, 夏中平, 陈善, 姜琳, 韩春. 甲状腺乳头状癌Delphian淋巴结转移的危险因素[J]. 外科理论与实践, 2022, 27(05): 453-457. |
| [8] | 王文涵, 夏蜀珺, 詹维伟. 长链非编码RNA ENST00000489676在超声评估甲状腺乳头状癌颈部淋巴结转移中的应用[J]. 诊断学理论与实践, 2022, 21(04): 514-519. |
| [9] | 徐琛莹, 李嫣然, 倪晓枫, 徐上妍, 林青. 超声预测老年甲状腺乳头状癌患者颈部淋巴结转移的效能及相关超声征象分析[J]. 诊断学理论与实践, 2022, 21(03): 343-348. |
| [10] | 刘荣耀, 李祥翠, 王丽娜, 陈海珍. 甲状腺乳头状癌颈部淋巴结转移的危险因素分析[J]. 外科理论与实践, 2022, 27(01): 76-79. |
| [11] | 唐娟, 刘志艳. 第4版WHO分化型甲状腺癌病理分类及其进展[J]. 外科理论与实践, 2021, 26(06): 504-509. |
| [12] | 王甜甜, 谢秋萍, 王平. 机器人甲状腺手术的颈侧区淋巴结清扫[J]. 外科理论与实践, 2021, 26(06): 476-481. |
| [13] | 刘威, 王聪, 王正林, 艾志龙. 单侧甲状腺乳头状癌Delphian淋巴结转移的发生率及其临床意义[J]. 外科理论与实践, 2021, 26(05): 445-448. |
| [14] | 况李君, 陶玲玲, 詹维伟, 李伟伟, 樊金芳, 周伟. 负压细针抽吸和毛细抽吸活检法穿刺洗脱液中甲状腺球蛋白测定在甲状腺乳头状癌淋巴结转移中的诊断价值比较[J]. 诊断学理论与实践, 2021, 20(04): 367-371. |
| [15] | 陈雪梅, 陈远洋, 周全红. 研究微重力对甲状腺肿瘤的影响[J]. 外科理论与实践, 2021, 26(02): 179-182. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||