诊断学理论与实践 ›› 2021, Vol. 20 ›› Issue (05): 466-470.doi: 10.16150/j.1671-2870.2021.05.008
李娟1,2( ), 刘劲松1,2, 李梅1,2, 李殿炜1,2, 朱弘1,2
), 刘劲松1,2, 李梅1,2, 李殿炜1,2, 朱弘1,2
收稿日期:2021-03-19
出版日期:2021-10-25
发布日期:2022-06-28
通讯作者:
李娟
E-mail:174363097@qq.com
LI Juan1,2(), LIU Jingsong1,2, LI Mei1,2, LI Dianwei1,2, ZHU Hong1,2
Received:2021-03-19
Online:2021-10-25
Published:2022-06-28
Contact:
LI Juan
E-mail:174363097@qq.com
摘要:
目的:探讨细支气管腺瘤的临床病理特征、诊断及鉴别诊断。 方法:收集六安市人民医院2020年1月至12月收治的10例细支气管腺瘤病例,总结其临床资料、影像学检查结果、组织病理学特征及免疫组织化学(免疫组化)表型。 结果:患者中男性4例,女性6例,发病年龄为49~79岁。大多患者均无明显临床症状,仅在胸部CT检查时发现肺部磨玻璃样结节。10例患者病灶均位于肺外周,切面大部分为灰白结节,质地中等或质地软,肿瘤与周围正常肺组织界限尚清楚。6例患者为近端型,4例患者为远端型。在光学显微镜下观察,肿瘤呈腺腔型、平坦型及乳头型结构,可见大量细胞外黏液,腔缘内衬细胞为黏液细胞、纤毛细胞、非纤毛立方细胞、Clara细胞,细胞无异型性及未见核分裂象,腔缘外可见连续的基底细胞层,部分肿瘤可无黏液细胞和纤毛细胞。免疫组化标志物p40、p63、CK5/6均在基底细胞层连续显示。 结论:细支气管腺瘤是一种由双层细胞构成的外周性肺肿瘤,诊断该疾病要求在病理检查中观察到完整的基底细胞层,明确诊断该病困难时,需进行免疫组化标志物(p40、p63和CK5/6)检测,明确基底细胞层的存在。
中图分类号:
李娟, 刘劲松, 李梅, 李殿炜, 朱弘. 细支气管腺瘤10例临床病理分析及文献复习[J]. 诊断学理论与实践, 2021, 20(05): 466-470.
LI Juan, LIU Jingsong, LI Mei, LI Dianwei, ZHU Hong. Bronchiolar adenoma: a clinic pathological analysis of 10 cases and review of literature[J]. Journal of Diagnostics Concepts & Practice, 2021, 20(05): 466-470.
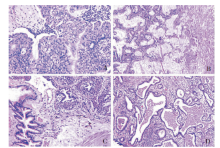
图1
近端型BA的病理学图(HE) A:见纤毛细胞性乳头(×200);B:腔缘细胞由丰富的黏液细胞和纤毛细胞组成,腔缘外为连续的基底细胞,周围黏液较丰富,可形成黏液湖(×100);C:肿瘤内可见部分残存的扩张的支气管(×200);D:肿瘤细胞沿肺泡壁平坦生长为主,腔缘细胞含有大量的纤毛(×100)。
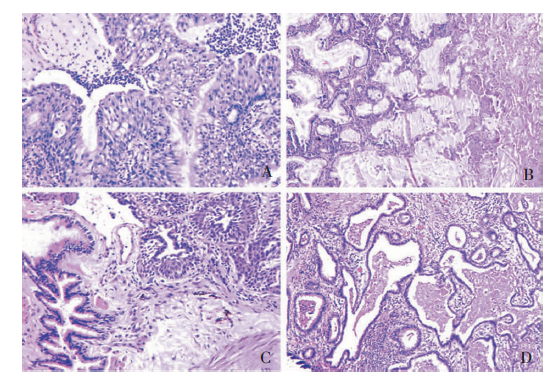
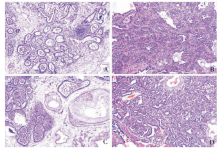
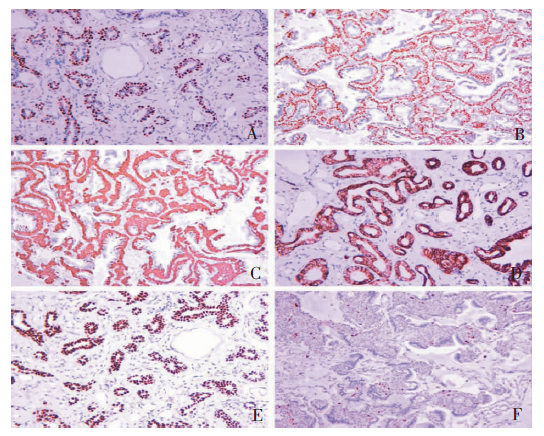
图2
远端型BA的病理学图(HE) A:扁平状,以腺管为主,腔缘细胞为立方状(×100);B:腔缘细胞外为连续的基底细胞,部分见基底细胞增生呈多层(×100);C:肿瘤旁或肿瘤内常可见小动脉(×100);D:部分腺腔形态不规则,腔缘细胞未见异型,腔缘外侧见基底细胞(×100)。
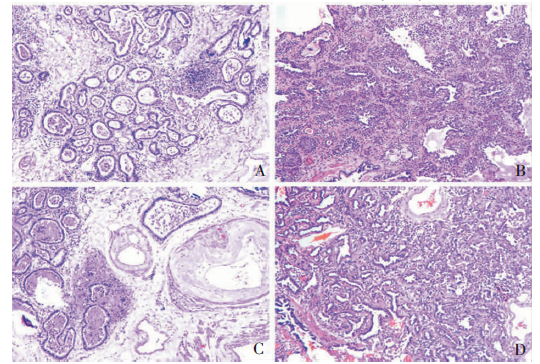
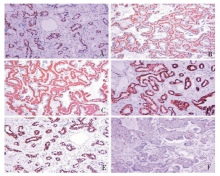
图3
BA的免疫组化染色图(EnVision) A:p40在基底细胞胞核中连续阳性表达(×100);B:p63在基底细胞细胞核中呈连续阳性表达(×100);C:CK5/6在基底细胞细胞质中呈连续阳性表达(×100);D:CK7在基底细胞及腔缘细胞细胞质中均呈阳性表达(×100, EnVision);E:TTF1在基底细胞及腔缘细胞细胞核均呈阳性表达(×100);F:Ki-67 在基底细胞、腔缘细胞细胞核中均为低表达(×100)
| [1] |
Chang JC, Montecalvo J, Borsu L, et al. Bronchiolar adenoma: expansion of the concept of ciliated muconodular papillary tumors with proposal for revised terminology based on morphologic, immunophenotypic, and genomic analysis of 25 cases[J]. Am J Surg Pathol, 2018,42(8):1010-1026.
doi: 10.1097/PAS.0000000000001086 URL |
| [2] | Ishikawa Y. Ciliated muconodular papillary tumor of the peripheral lung: benign or malignant?[J]. Pathol Clin Med, 2002,20:964-965. |
| [3] | 王恩华. 细支气管腺瘤:易与癌混淆的良性肿瘤[J]. 中华病理学杂志, 2019,48(6):425-432. |
| [4] |
Sasaki E, Masago K, Fujita S, et al. AKT1 mutations in peripheral bronchiolar papilloma: glandular papilloma and mixed squamous cell and glandular papilloma is di-stinct from bronchiolar adenoma[J]. Am J Surg Pathol, 2021,45(1):119-126.
doi: 10.1097/PAS.0000000000001573 URL |
| [5] | 张杰, 邵晋晨, 韩昱晨, 等. 细支气管腺瘤病理诊断若干问题[J]. 中华病理学杂志, 2020,49(6):529-533. |
| [6] |
Jin Y, Shen X, Shen L, et al. Ciliated muconodular papillary tumor of the lung harboring ALK gene rearrangement: Case report and review of the literature[J]. Pathol Int, 2017,67(3):171-175.
doi: 10.1111/pin.12512 URL |
| [7] |
Shao K, Wang Y, Xue Q, et al. Clinicopathological features and prognosis of ciliated muconodular papillary tumor[J]. J Cardiothorac Surg, 2019,14(1):143.
doi: 10.1186/s13019-019-0962-3 URL |
| [8] |
Liu L, Aesif SW, Kipp BR, et al. Ciliated muconodular papillary tumors of the lung can occur in western patients and show mutations in BRAF and AKT1[J]. Am J Surg Pathol, 2016,40(12):1631-1636.
doi: 10.1097/PAS.0000000000000707 URL |
| [9] |
Liu S, Liu N, Xiao M, et al. First case of bronchiolar adenoma lined purely by mucinous luminal cells with molecu-lar analysis: a case report[J]. Medicine (Baltimore), 2020, 99(39):e22322.
doi: 10.1097/MD.0000000000022322 URL |
| [10] |
Sun Y, Liu M, Jiang Z, et al. Bronchiolar adenoma with diffuse pulmonary nodules: a extremely rare case report and review of literature[J]. BMC Pulm Med, 2020,20(1):192.
doi: 10.1186/s12890-020-01228-1 URL |
| [11] |
Cao L, Wang Z, Gong T, et al. Discriminating between bronchiolar adenoma, adenocarcinoma in situ and minimally invasive adenocarcinoma of the lung with CT[J]. Diagn Interv Imaging, 2020,101(12):831-837.
doi: 10.1016/j.diii.2020.05.005 URL |
| [12] |
Abe M, Osoegawa A, Miyawaki M, et al. Ciliated muco-nodular papillary tumor of the lung: a case report and li-terature review[J]. Gen Thorac Cardiovasc Surg, 2020,68(11):1344-1349.
doi: 10.1007/s11748-019-01252-x URL |
| [13] |
Tachibana M, Saito M, Kobayashi J, et al. Distal-type bronchiolar adenoma of the lung expressing p16 INK4a - morphologic, immunohistochemical, ultrastructural and genomic analysis - report of a case and review of the lite-rature[J]. Pathol Int, 2020,70(3):179-185.
doi: 10.1111/pin.12904 URL |
| [1] | 车稳, 柳蒋书, 陈晓炎, 王朝夫, 袁菲, 王璇. 肺混合性鳞状细胞和腺性乳头状瘤2例临床病理特征及冷冻切片病理诊断误诊分析[J]. 诊断学理论与实践, 2022, 21(04): 476-481. |
| [2] | 王昭晖, 吴海波. 胃神经鞘瘤31例临床病理学分析[J]. 诊断学理论与实践, 2021, 20(06): 552-556. |
| [3] | 吴冬梅, 吴丽莉, 陈佳, 刘坤. 淋巴上皮样肝细胞肝癌一例报告附文献复习[J]. 诊断学理论与实践, 2021, 20(05): 498-501. |
| [4] | 韦若蕖, 余红, 姚志荣. 儿童成纤维细胞结缔组织痣一例报道并文献复习[J]. 诊断学理论与实践, 2021, 20(02): 190-194. |
| [5] | 孟磊俊, 张晶, 王雪莉, 李治, 张泓, 曾乃燕. 儿童伯基特淋巴瘤中差异表达基因的鉴定及临床应用[J]. 诊断学理论与实践, 2020, 19(03): 248-257. |
| [6] | 何燕燕, 冯砅锦, 蔚青. 前列腺多形性巨细胞腺癌一例报告及文献复习[J]. 诊断学理论与实践, 2019, 18(2): 160-164. |
| [7] | 金娇莺, 李倩玉, 蒋虹伟, 韩冬艳, 奚豪, 蔚青. 混合性嗜铬细胞瘤1例报道并文献复习[J]. 诊断学理论与实践, 2019, 18(2): 165-169. |
| [8] | 王顺利, 邓双双, 高慧, 肖天羽, 高金莉. 乳腺包裹性乳头状癌的临床和病理特征分析[J]. 诊断学理论与实践, 2019, 18(1): 89-92. |
| [9] | 刘立伟, 杨晓群, 范德生. 宫颈肝样腺癌一例报告及文献复习[J]. 诊断学理论与实践, 2019, 18(06): 680-682. |
| [10] | 肖辅国, 潘自来. 浸润前病变的CT值变化在鉴别肺纯磨玻璃结节性质的价值探讨[J]. 诊断学理论与实践, 2019, 18(05): 521-525. |
| [11] | 韩冬艳, 付慧君, 何燕燕, 奚豪, 蔚青. 内淋巴囊肿瘤临床病理分析及文献复习[J]. 诊断学理论与实践, 2018, 17(06): 711-714. |
| [12] | 朱培培, 邹珏, 陈军, 徐蓉蓉, 颜红柱. 颅内孤立性纤维性肿瘤/血管周细胞瘤20例临床病理特征分析[J]. 诊断学理论与实践, 2017, 16(06): 622-626. |
| [13] | 许海敏, 张培培. 三款自动免疫组织化学染色仪在乳腺癌病理诊断中的应用比较[J]. 诊断学理论与实践, 2017, 16(06): 645-649. |
| [14] | 符蓉, 王朝夫, 欧阳斌燊. 软骨母细胞瘤21例临床病理及影像学特征分析[J]. 诊断学理论与实践, 2017, 16(05): 537-539. |
| [15] | 顾青, 潘晓林, 赵艳. 转移相关基因1蛋白在子宫颈病变组织中的表达及临床意义[J]. 诊断学理论与实践, 2017, 16(03): 333-337. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||