诊断学理论与实践 ›› 2022, Vol. 21 ›› Issue (01): 74-79.doi: 10.16150/j.1671-2870.2022.01.014
杨伯文, 姜美娇, 陈慧( )
)
出版日期:2022-02-25
发布日期:2022-02-25
通讯作者:
陈慧
E-mail:ch11516@rjh.com.cn
基金资助:
YANG Bowen, JIANG Meijiao, CHEN Hui()
Online:2022-02-25
Published:2022-02-25
Contact:
CHEN Hui
E-mail:ch11516@rjh.com.cn
摘要:
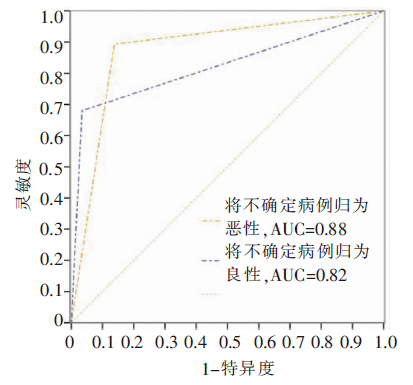
目的: 在中国人群中行单中心试验来验证国际卵巢肿瘤分析组织(International Ovarian Tumour Analysis,IOTA)简单法(simple rules,SR)在术前鉴别卵巢肿瘤良恶性的价值。目的: 选取2017年5月至12月上海交通大学医学院附属瑞金医院妇产科收治的卵巢肿块患者278例,共278个肿块,术前予行超声检查,并统计SR给出的拟诊。拟诊结果包括良性(175例)、恶性(交界性归为恶性,75例)、不确定(37例)。以病理学结果为金标准,计算SR鉴别卵巢肿瘤良恶性灵敏度、特异度和受试者操作特征(receiver operator characteristic,ROC)曲线下面积。结果: 术后病理提示,本组良性病例为203例,恶性病例为75例。SR能正确检出86.2%(175/203)的良性肿瘤,正确检出68.0%(51/75)的恶性肿瘤,15例为漏诊或误诊,37例未能给出诊断。在SR的超声特征中,M4(不规则多房囊实性肿块,最大径≥100 mm)预测恶性肿瘤的准确率最高(90.5%);B3(声影)对良性肿瘤的预测价值最高(准确率为100.0%)。去除不确定的37例病例,在241例患者中,SR的诊断恶性卵巢肿瘤的灵敏度为86.4%、特异度为96.2%。在278例患者中,如将获得不确定SR结论的肿块归类为恶性,SR诊断恶性卵巢肿瘤的灵敏度为89.3%,特异度为86.2%,ROC曲线下面积0.88;将不确定肿块归类为良性时,诊断恶性卵巢肿瘤的灵敏度为68.0%,特异度为96.6%,ROC曲线下面积0.82,2种方法间差异有统计学(P=0.04)。8例病理检查结果为恶性而超声检查提示良性,回顾总结超声图像,发现当囊性肿块内壁不光滑,附壁见乳头状突起,或囊性肿块直径大于10 cm时,需考虑肿块有恶性的可能性。7例病理检查结果为良性而超声检查提示恶性,回顾超声图像,发现肿块实性部分存在血供,血流分级2~3级时,需考虑肿块有良性的可能性。结论: SR使用简单、便捷,适于中国人群应用;将SR不确定分类结果计入恶性,此时诊断恶性卵巢肿瘤灵敏度较高。
中图分类号:
杨伯文, 姜美娇, 陈慧. 超声IOTA简单法鉴别诊断卵巢肿瘤良恶性的临床研究[J]. 诊断学理论与实践, 2022, 21(01): 74-79.
YANG Bowen, JIANG Meijiao, CHEN Hui. Study on differential diagnosis of malignant and benign ovarian tumors through IOTA simple rules[J]. Journal of Diagnostics Concepts & Practice, 2022, 21(01): 74-79.
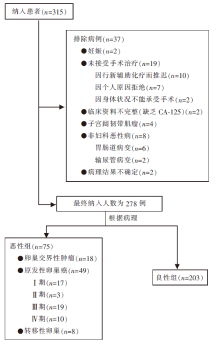
图1
病例筛选流程图
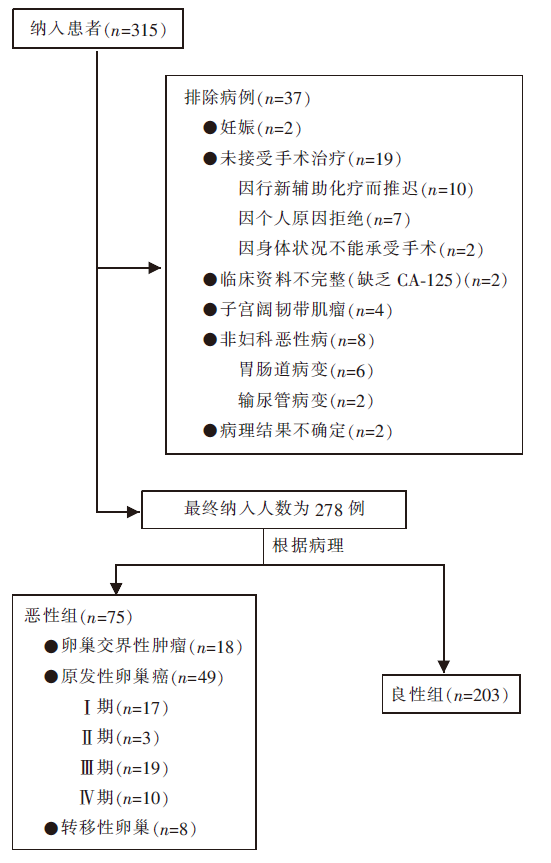

图2
简单法良性和恶性超声特征 良性征像,B1:单房囊肿;B2:肿块含实性成分,实性成分最大径<7 mm;B3:声影;B4:平滑的多房囊肿,囊肿最大径<100 mm;B5:无血流信号。恶性征像,M1:不规则实性肿块;M2:腹水;M3:乳头状突起≥4枚;M4:不规则的多房囊实性肿块,囊肿最大径≥100 mm;M5:丰富血流信号。
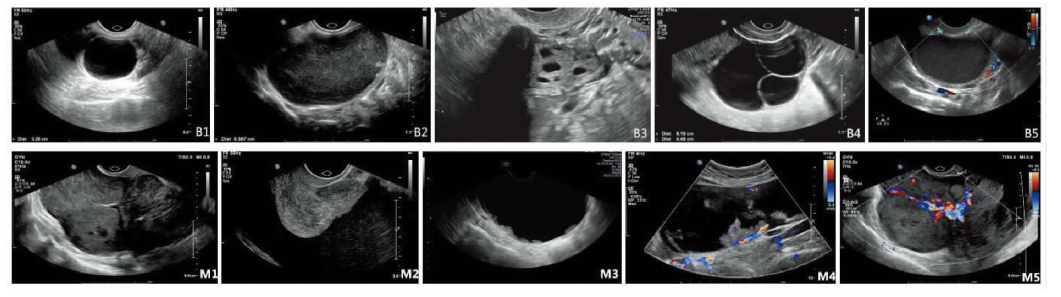
表1
SR对不同组织学类型卵巢肿瘤的评估比较[n(%)]
| 组织学类型 | 例数 (n) | SR未能分类 | SR分类 | |
|---|---|---|---|---|
| 分类正确 | 分类错误 | |||
| 良性 | 203 | 21(10.3) | 175(86.2) | 7(3.5) |
| 恶性 | ||||
| 交界性 | 18 | 7(38.9) | 7(38.9) | 4(22.2) |
| 原发恶性 | 49 | 8(16.3) | 37(75.5) | 4(8.2) |
| 转移癌 | 8 | 1(12.5) | 7(87.5) | - |
| 总计 | 278 | 37(13.3) | 226(81.3) | 15(5.4) |
表2
卵巢良、恶性肿瘤患者临床和超声特征比较[中位数(四分位数范围),例(n)]
| 指标 | 良性(n=203) | 恶性(n=75) | P值 |
|---|---|---|---|
| 临床资料 | |||
| 年龄(岁) | 41(14~83) | 51(20~84) | <0.001 |
| 绝经状态(绝经前/后) | 145/58 | 35/40 | <0.001 |
| CA125(U/mL) | 18(5~1 672) | 68(5~10 000) | <0.001 |
| 卵巢癌家族史 | 1(0.5%) | 2(2.7%) | 0.178 |
| 超声特征 | |||
| 病灶最大径(mm) | 55(16~252) | 75(21~294) | <0.001 |
| 实性成分 | |||
| 存在实性成分 | 57(28.1%) | 66(88.0%) | <0.001 |
| 实性成分最大径(mm) | 24(3~132) | 53(5~166) | <0.001 |
| 乳头状突起 | |||
| >0* | 21(10.3%) | 25(33.3%) | <0.001 |
| 0 | 182(89.7%) | 50(66.7%) | |
| 1 | 12(5.9%) | 7(9.3%) | |
| 2 | 2(1.0%) | 3(4.0%) | |
| 3 | 2(1.0%) | 3(4.0%) | |
| >3 | 5(2.5%) | 12(16.0%) | |
| 病灶彩色多普勒血流 | |||
| 1级 | 159(78.3%) | 8(10.7%) | <0.001 |
| 2级 | 27(13.3%) | 23(30.7%) | |
| 3级 | 11(5.4%) | 18(24.0%) | |
| 4级 | 6(3.0%) | 26(34.7%) | |
| 肿块类型 | |||
| 单房囊性 | 99(48.8%) | 2(2.7%) | <0.001 |
| 单房囊实性 | 26(12.8%) | 18(24.0%) | 0.023 |
| 多房囊性 | 48(23.6%) | 7(9.3%) | 0.008 |
| 多房囊实性 | 14(6.9%) | 24(32.0%) | <0.001 |
| 实性 | 16(7.9%) | 24(32.0%) | <0.001 |
| 声影 | 24(11.8%) | 0(0) | 0.002 |
| 腹水 | 3(1.5%) | 24(32.0%) | <0.001 |
表3
SR超声特征预测卵巢肿瘤良恶性的诊断价值
| 超声特征 | 例数(n/n) | 预测价值(95%CI) |
|---|---|---|
| 恶性超声特征(M) | ||
| M1 | 23/31 | 74.2%(57.9%~90.5%) |
| M2 | 24/27 | 88.9%(76.2%~100.0%) |
| M3 | 12/17 | 70.6%(46.4%~94.7%) |
| M4 | 19/21 | 90.5%(76.8%~100.0%) |
| M5 | 26/32 | 81.3%(67.0%~95.5%) |
| 良性超声特征(B) | ||
| B1 | 99/101 | 98.0%(95.3%~100.0%) |
| B2 | 4/5 | 80.0%(24.5%~100.0%) |
| B3 | 24/24 | 100.0%(100.0%~100.0%) |
| B4 | 36/39 | 92.3%(83.6%~100.0%) |
| B5 | 159/167 | 95.2%(91.9%~98.5%) |
表4
SR鉴别卵巢肿瘤良恶性的诊断效能
| 组别 | 灵敏度 [%(95%CI)] | 特异度 [%(95%CI)] | 阳性预测值 [%(95%CI)] | 阴性预测值 [%(95%CI)] | 阳性似然比 (95%CI) | 阴性似然比 (95%CI) | 诊断比值比 |
|---|---|---|---|---|---|---|---|
| 方法一(n=278) | 89.3(80~95) | 86.2(81~90) | 70.5(60~79) | 95.6(91~98) | 6.5(5~9) | 0.1(0~1) | 54.0 |
| 方法二(n=278) | 68.0(56~78) | 96.6(93~98) | 87.9(76~95) | 89.1(84~93) | 19.7(9~42) | 0.3(0~1) | 59.8 |
| 方法三(n=241) | 86.4(74~94) | 96.2(92~98) | 87.9(76~95) | 95.6(91~98) | 22.5(11~48) | 0.1(0~1) | 160.5 |
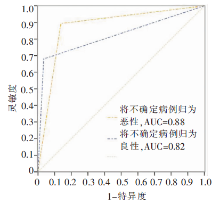
图3
SR鉴别卵巢肿瘤良恶性ROC曲线
| [1] |
Buys SS, Partridge E, Black A, et al. Effect of screening on ovarian cancer mortality: the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Randomized Controlled Trial[J]. JAMA, 2011, 305(22):2295-2303.
doi: 10.1001/jama.2011.766 URL |
| [2] |
Alcázar JL, Royo P, Jurado M, et al. Triage for surgical management of ovarian tumors in asymptomatic women: assessment of an ultrasound-based scoring system[J]. Ultrasound Obstet Gynecol, 2008, 32(2):220-225.
doi: 10.1002/uog.5401 pmid: 18618475 |
| [3] |
Basha MAA, Metwally MI, Gamil SA, et al. Comparison of O-RADS, GI-RADS, and IOTA simple rules regarding malignancy rate, validity, and reliability for diagnosis of adnexal masses[J]. Eur Radiol, 2021, 31(2):674-684.
doi: 10.1007/s00330-020-07143-7 URL |
| [4] | 杨文敏, 吕国荣, 陈秋月. 卵巢-附件报告及数据系统、妇科影像报告与数据系统和简单法则风险预测模型鉴别诊断卵巢良、恶性肿瘤[J]. 中国医学影像技术, 2021, 37(9):1368-1372. |
| Yang W M, LV G R, Chen Q Y. Ovarian accessory report and data system, gynecological image report and data system and simple rule risk prediction model for differential diagnosis of benign and malignant ovarian tumors[J]. Chin Med Imaging technol, 2021, 37(9):1368-1372. | |
| [5] |
Timmerman D, Testa AC, Bourne T, et al. Simple ultrasound-based rules for the diagnosis of ovarian cancer[J]. Ultrasound Obstet Gynecol, 2008, 31(6):681-690.
doi: 10.1002/uog.5365 pmid: 18504770 |
| [6] |
van Calster B, Van Hoorde K, Valentin L, et al. Evalua-ting the risk of ovarian cancer before surgery using the ADNEX model to differentiate between benign, borderline, early and advanced stage invasive, and secondary metastatic tumours: prospective multicentre diagnostic study[J]. BMJ, 2014, 349:g5920.
doi: 10.1136/bmj.g5920 URL |
| [7] | Royal College of Obstetricians and Gynaecologists. Mana-gement of suspected ovarian masses in premenopausal women[R/OL]. Green-top guideline No 62. RCOG, Nov 2011-11 [2022-01-25]. https://www.rcog.org.uk/files/rcog-corp/GTG62_021211_OvarianMasses.pdf. |
| [8] |
American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Gynecology. Practice Bulletin No. 174: Evaluation and Management of Adnexal Masses[J]. Obstet Gynecol. 2016, 128(5):e210-e226.
doi: 10.1097/AOG.0000000000001768 URL |
| [9] |
Glanc P, Benacerraf B, Bourne T, et al. First International Consensus Report on Adnexal Masses: Management Recommendations[J]. J Ultrasound Med, 2017, 36(5):849-863.
doi: 10.1002/jum.14197 URL |
| [10] |
Timmerman D, Valentin L, Bourne TH, et al. Terms, definitions and measurements to describe the sonographic features of adnexal tumors: a consensus opinion from the International Ovarian Tumor Analysis IOTA Group[J]. Ultrasound Obstet Gynecol, 2000, 16(5):500-505.
doi: 10.1046/j.1469-0705.2000.00287.x URL |
| [11] |
Meys EMJ, Jeelof LS, Achten NMJ, et al. Estimating risk of malignancy in adnexal masses: external validation of the ADNEX model and comparison with other frequently used ultrasound methods[J]. Ultrasound Obstet Gynecol, 2017, 49(6):784-792.
doi: 10.1002/uog.17225 pmid: 27514486 |
| [12] |
Meinhold-Heerlein I, Fotopoulou C, Harter P, et al. The new WHO classification of ovarian, fallopian tube, and primary peritoneal cancer and its clinical implications[J]. Arch Gynecol Obstet, 2016, 293(4):695-700.
doi: 10.1007/s00404-016-4035-8 pmid: 26894303 |
| [13] |
Prat J. FIGO Committee on Gynecologic Oncology. FIGO′s staging classification for cancer of the ovary, fallopian tube, and peritoneum: abridged republication[J]. J Gynecol Oncol, 2015, 26(2):87-89.
doi: 10.3802/jgo.2015.26.2.87 URL |
| [14] |
Andreotti RF, Timmerman D, Benacerraf BR, et al. Ovarian-Adnexal Reporting Lexicon for Ultrasound: A White Paper of the ACR Ovarian-Adnexal Reporting and Data System Committee[J]. J Am Coll Radiol, 2018, 15(10):1415-1429.
doi: S1546-1440(18)30839-1 pmid: 30149950 |
| [15] |
Nunes N, Ambler G, Foo X, et al. Use of IOTA simple rules for diagnosis of ovarian cancer: meta-analysis[J]. Ultrasound Obstet Gynecol, 2014, 44(5):503-514.
doi: 10.1002/uog.13437 pmid: 24920435 |
| [16] |
Ruiz de Gauna B, Rodriguez D, Olartecoechea B, et al. Diagnostic performance of IOTA simple rules for adnexal masses classification: a comparison between two centers with different ovarian cancer prevalence[J]. Eur J Obstet Gynecol Reprod Biol, 2015, 191:10-14.
doi: 10.1016/j.ejogrb.2015.05.024 URL |
| [17] |
Timmerman D, Ameye L, Fischerova D, et al. Simple ultrasound rules to distinguish between benign and malignant adnexal masses before surgery: prospective validation by IOTA group[J]. BMJ, 2010, 341:c6839.
doi: 10.1136/bmj.c6839 URL |
| [18] |
刘真真, 石志敏, 徐钟慧, 等. IOTA ADNEX模型与简单法则对附件区疑难病变的诊断价值[J]. 中华医学超声杂志(电子版), 2020, 17(11):1084-1089.
doi: 10.3877/cma.j.issn.1672-6448.2020.11.005 |
| Liu Z Z, Shi Z M, Xu Z H, et al. Diagnostic value of iota adnex model and simple rule in difficult lesions of accessory region[J]. Chin J Med Ultrasound (Electronic Edition), 2020, 17(11):1084-1089. | |
| [19] |
Ameye L, Timmerman D, Valentin L, et al. Clinically oriented three-step strategy for assessment of adnexal pathology[J]. Ultrasound Obstet Gynecol, 2012, 40(5):582-591.
doi: 10.1002/uog.11177 pmid: 22511559 |
| [20] |
Brown DL, Dudiak KM, Laing FC. Adnexal masses: US characterization and reporting[J]. Radiology, 2010, 254(2):342-354.
doi: 10.1148/radiol.09090552 URL |
| [21] |
Sayasneh A, Ekechi C, Ferrara L, et al. The characteristic ultrasound features of specific types of ovarian patho-logy (review)[J]. Int J Oncol, 2015, 46(2):445-458.
doi: 10.3892/ijo.2014.2764 pmid: 25406094 |
| [22] |
Timmerman D, Van Calster B, Testa A, et al. Predicting the risk of malignancy in adnexal masses based on the Simple Rules from the International Ovarian Tumor Analysis group[J]. Am J Obstet Gynecol, 2016, 214(4):424-437.
doi: S0002-9378(16)00009-0 pmid: 26800772 |
| [23] |
Valentin L, Ameye L, Savelli L, et al. Unilocular adnexal cysts with papillary projections but no other solid components: is there a diagnostic method that can classify them reliably as benign or malignant before surgery?[J]. Ultrasound Obstet Gynecol, 2013, 41(5):570-581.
doi: 10.1002/uog.12294 pmid: 22915541 |
| [24] |
Landolfo C, Valentin L, Franchi D, et al. Differences in ultrasound features of papillations in unilocular-solid adnexal cysts: a retrospective international multicenter study[J]. Ultrasound Obstet Gynecol, 2018, 52(2):269-278.
doi: 10.1002/uog.18951 pmid: 29119698 |
| [1] | 刁雪红, 申艳, 陈林, 詹嘉, 方靓, 蔡剑飞, 陈悦. 超声微血流成像技术在临床缓解期类风湿性关节炎诊断中的应用[J]. 诊断学理论与实践, 2022, 21(05): 575-580. |
| [2] | 王之倩, 李敏, 于一飞, 周建桥. 21-羟化酶缺陷先天性肾上腺皮质增生患者睾丸肾上腺残基瘤超声特征分析[J]. 诊断学理论与实践, 2022, 21(05): 588-591. |
| [3] | 顾炫, 柳俊. 超声筛查鉴别胰腺实性假乳头状瘤与胰腺导管腺癌的研究分析[J]. 诊断学理论与实践, 2022, 21(04): 504-508. |
| [4] | 王文涵, 夏蜀珺, 詹维伟. 长链非编码RNA ENST00000489676在超声评估甲状腺乳头状癌颈部淋巴结转移中的应用[J]. 诊断学理论与实践, 2022, 21(04): 514-519. |
| [5] | 何新, 陈慧, 冯炜炜. 机器学习算法在辅助超声诊断附件肿块良恶性中的应用研究进展[J]. 诊断学理论与实践, 2022, 21(04): 541-546. |
| [6] | 杜燕然, 焦景, 任芸芸, 周建桥. 超声影像组学技术在评估胎肺成熟度中的应用[J]. 诊断学理论与实践, 2022, 21(03): 326-330. |
| [7] | 桂燕萍, 陈晔芬, 施仲伟, 许燕. 超声心动图右室面积变化分数筛查左心室射血分数降低的心力衰竭患者心脏同步性研究[J]. 诊断学理论与实践, 2022, 21(03): 331-335. |
| [8] | 徐琛莹, 李嫣然, 倪晓枫, 徐上妍, 林青. 超声预测老年甲状腺乳头状癌患者颈部淋巴结转移的效能及相关超声征象分析[J]. 诊断学理论与实践, 2022, 21(03): 343-348. |
| [9] | 王晨琛, 方跃华, 施仲伟, 屈雪蒸. 25例主动脉瓣成形术后一年的超声心动图评价[J]. 诊断学理论与实践, 2022, 21(03): 395-398. |
| [10] | 周建桥. 分布式云超声:超声成像系统研发的新路径[J]. 诊断学理论与实践, 2022, 21(01): 38-40. |
| [11] | 曹云云, 王冠杰, 曾敏, 王海飞, 牛建梅, 周雷平. 早孕期超声相关参数预测胚胎妊娠结局价值的分析[J]. 诊断学理论与实践, 2021, 20(05): 445-449. |
| [12] | 何碧媛, 周毓青, 姚秉彝, 曹力, 包丽. 中孕期弹性超声成像宫颈机能智能定量分析预测自发性早产的临床应用价值[J]. 诊断学理论与实践, 2021, 20(05): 450-455. |
| [13] | 杨田, 吉翔, 牛建梅, 孔晓晓, 吕明丽. 二维超声在产前胎儿胸腺发育评估中的应用[J]. 诊断学理论与实践, 2021, 20(05): 471-474. |
| [14] | 赵然, 詹维伟, 柳俊. 三维超声监测特发性低促性腺激素性性腺功能减退症无精子患者睾丸体积对患者生精功能的预测价值[J]. 诊断学理论与实践, 2021, 20(03): 279-283. |
| [15] | 钱乐, 姜美娇, 杨伯文, 陈慧. 卵巢囊性腺纤维瘤和卵巢腺纤维瘤的超声诊断效能及图像特征分析[J]. 诊断学理论与实践, 2021, 20(02): 161-167. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||