诊断学理论与实践 ›› 2023, Vol. 22 ›› Issue (02): 178-183.doi: 10.16150/j.1671-2870.2023.02.012
李丽娟1,2, 谢洁2, 张文1,2, 马骏1,2( )
)
收稿日期:2023-02-19
出版日期:2023-04-25
发布日期:2023-08-31
通讯作者:
马骏 E-mail: jiangpuma@163.com
基金资助:
LI lijuan1,2, XIE Jie2, ZHANG Wen1,2, MA Jun1,2()
Received:2023-02-19
Online:2023-04-25
Published:2023-08-31
摘要:
Gitelman综合征(Gitelman syndrome, GS)是较少见的遗传性肾小管病,患者临床表现通常较轻,多为乏力、嗜盐、心悸等非特异性症状。GS继发横纹肌溶解症(rhabdomyolysis, RM)十分罕见,目前国内外文献报道仅10余例,且多见于儿童。本文报道了1例成人GS继发RM患者的详细诊治过程,并结合文献分析该疾病的诊治要点。该例患者为青年男性,长期存在不明原因的低钾血症,入院前因劳累出汗后,出现乏力加重伴肌肉酸痛。实验室检查提示患者存在低血钾、低血镁、代谢性碱中毒、低尿钙,肾素-血管紧张素-醛固酮系统轻度激活,伴肌酸激酶升高超过正常上限5倍。进一步行全外显子基因检测,结果提示该患者存在SLC12A3基因复合杂合突变,最终确诊该患者为GS继发RM。予口服安体舒通、氯化钾、钙镁片等补钾、补镁及水化治疗后,患者的临床症状明显好转。随访1年,患者的电解质水平基本正常,肾功能稳定。复习相关文献,发现GS患者继发RM临床罕见,且主要发生于严重低钾、低镁的儿童,常有剧烈运动、腹泻、服用药物等诱因,治疗不及时可出现肾功能衰竭等严重并发症。本病例提示成人GS患在一定诱因下亦可继发RM等严重症状,临床医师应掌握GS的诊治要点以减少漏诊、误诊。
中图分类号:
李丽娟, 谢洁, 张文, 马骏. Gitelman综合征继发横纹肌溶解症一例并文献复习[J]. 诊断学理论与实践, 2023, 22(02): 178-183.
LI lijuan, XIE Jie, ZHANG Wen, MA Jun. Gitelman syndrome complicated with rhabdomyolysis: a case report and literature review[J]. Journal of Diagnostics Concepts & Practice, 2023, 22(02): 178-183.
表1
患者实验室结果
| 项目 | 结果 | 参考范围 |
|---|---|---|
| 血钾 (mmol/L) | 1.7 | 3.5~5.5 |
| 血钠(mmol/L) | 141 | 130~147 |
| 血氯(mmol/L) | 102 | 96~108 |
| 血钙 (mmol/L) | 2.04 | 2~2.75 |
| 血镁 (mmol/L) | 0.52 | 0.74~1.03 |
| 血二氧化碳(mmol/L) | 27.2 | 21.0~31.0 |
| 肌酐(μmol/L) | 88 | 64~104 |
| 肌酸激酶(IU/L) | 1 707 | 22~269 |
| 肌酸激酶同工酶 (ng/mL) | 38.1 | 0.3~4 |
| 肌红蛋白 (ng/mL) | 586.6 | <70 |
| 肌钙蛋白I(ng/mL) | 0.035 | <0.040 |
| 血气分析 | ||
| pH | 7.453 | 7.350~7.450 |
| PCO2 (mmHg) | 41.3 | 350~450 |
| 碳酸氢根(HCO3-)(mmol/L) | 28.9 | 220~260 |
| 标准碱剩余 (mmol/L) | 4.9 | -30~30 |
| 24 h尿电解质 | ||
| 尿钾(mmol/24 h) | 110.40 | 36.00~90.00 |
| 尿钠(mmol/24 h) | 584.20 | 137.00~257.00 |
| 尿钙(mmol/24 h) | 1.9 | 2.5~7.5 |
| 尿镁 (mmol/24 h) | 8.74 | 3.00~5.00 |
| 尿氯(mmol/24 h) | 685.40 | 170~250 |
| 尿钾排泄分数(%) | 37 | 8~12 |
| 尿镁排泄分数(%) | 17.1 | <1.00 |
| 24 h尿肌酐(mmol/24 h) | 8.62 | |
| 尿钙/尿肌酐 | 0.22 | |
图1
SLC12A3 基因测序图 (A 患者,B 父亲,C 母亲)
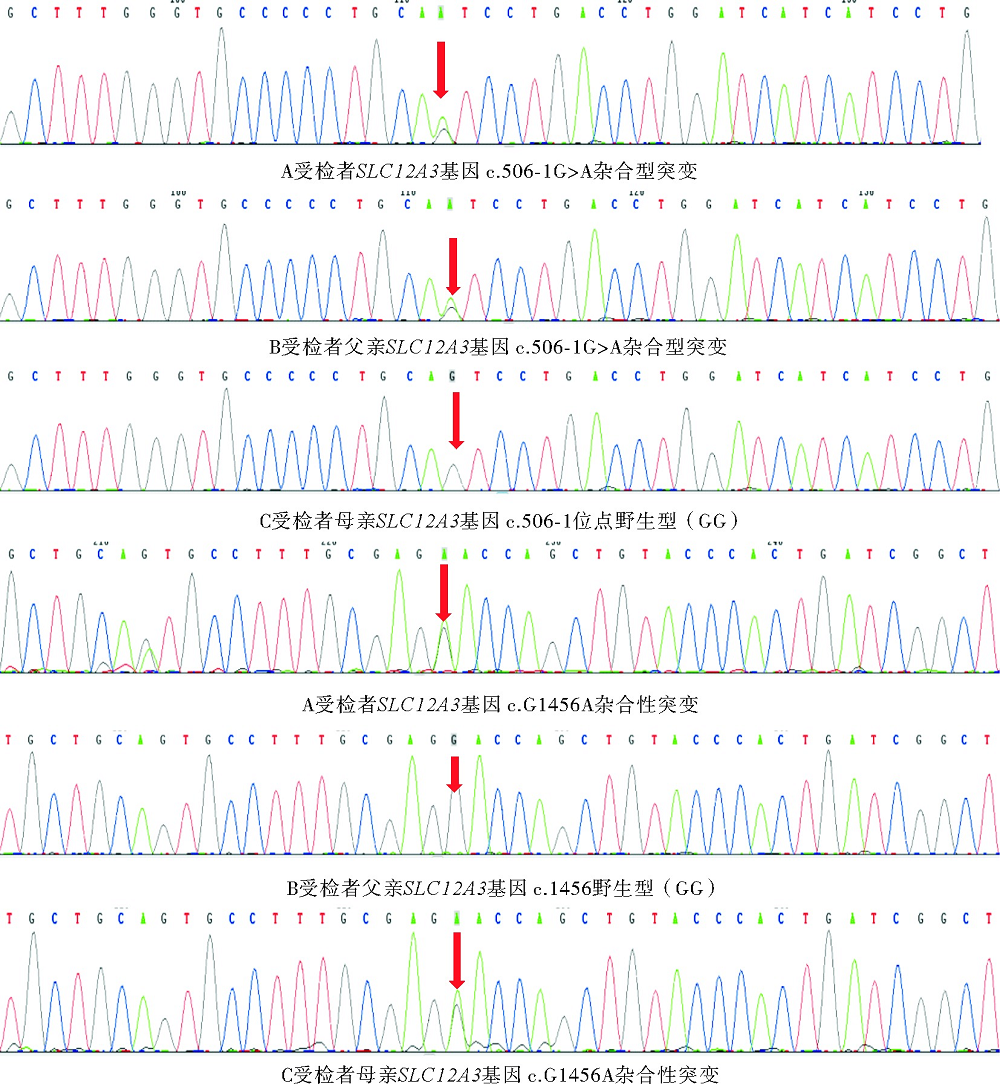
表2
文献报道中GS继发RM患者的临床特征
| 病例 | 性别 | 年龄(岁) | 诱因 | 临床表现 | 血钾(mmol/L) | 血镁(mmol/L) | CK(IU/L) | 基因诊断 | 参考文献 |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 女 | 21 | 病毒性肠炎 | 下肢乏力、肌肉痛 | 1.9 | 0.53 | 1454 | 是 | |
| 2 | 男 | 18 | 流感样症状 | 肌肉痛、行走困难 | 3.7 | / | / | / | |
| 3 | 男 | 15 | / | 严重肌无力和肌肉抽搐 | 2.1 | / | / | / | |
| 4 | 女 | 13 | / | 肢体乏力、肌痛、行走困难 | 2.1 | 0.79 | 1248 | 是 | |
| 5 | 男 | 62 | 甘草 | 肢体乏力、肌痛、尿色深 | 1.84 | 0.68 | 10117 | 是 | |
| 6 | 男 | 14 | / | 肢体麻木、疲劳、发作性抽搐 | 2.41 | 0.57 | 31567 | 是 | |
| 7 | 男 | 15 | 剧烈运动 | 四肢酸痛、乏力 | 2.8 | 0.62 | 3365 | 是 | |
| 8 | 男 | 14 | 剧烈运动 | 双下肢疼痛 | 3.39 | 0.66 | 4934 | 是 | |
| 9 | 男 | 25 | 剧烈运动 | 全身肌肉疼痛 | 2.8 | 0.49 | 8000 | 是 | |
| 10 | 女 | 16 | 剧烈运动 | 下肢肌痛、乏力 | 3.45 | 0.51 | 2398 | 是 | |
| 11 | 男 | 13 | 剧烈运动 | 下肢疼 | 2.42 | 0.52 | 7000 | 是 | |
| 12 | 男 | 19 | 劳累 | 四肢乏力酸痛 | 1.34 | 0.76 | 19018 | 是 |
| [1] | 中国研究型医院学会罕见病分会, 中国罕见病联盟, 北京罕见病诊疗与保障学会, 等. Gitelman综合征诊疗中国专家共识(2021版)[J]. 罕见病研究, 2022, 1(1):56-67. |
| Rare Diseases Society of Chinese Research Hospital Association, China Alliance for Rare Disease, Beijing So-ciety of Rare Disease Clinical Care and Accessibility, Gitelman Syndrome Consensus Working Group. Expert consensus for the diagnosis and treatment of gitelman syndrome in China ( 2021)[J]. J Rare Dis, 2022, 1(1):56-67. | |
| [2] |
MELLI G, CHAUDHRY V, CORNBLATH D R. Rhabdomyolysis: an evaluation of 475 hospitalized patients[J]. Medicine (Baltimore), 2005, 84(6):377-385.
doi: 10.1097/01.md.0000188565.48918.41 URL |
| [3] |
BLANCHARD A, BOCKENHAUER D, BOLIGNANO D, et al. Gitelman syndrome: consensus and guidance from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference[J]. Kidney Int, 2017, 91(1):24-33.
doi: S0085-2538(16)30602-0 pmid: 28003083 |
| [4] |
HSU Y J, YANG S S, CHU N F, et al. Heterozygous mutations of the sodium chloride cotransporter in Chinese children: prevalence and association with blood pressure[J]. Nephrol Dial Transplant, 2009, 24(4):1170-1175.
doi: 10.1093/ndt/gfn619 URL |
| [5] |
KNOERS N V, LEVTCHENKO E N. Gitelman syndrome[J]. Orphanet J Rare Dis, 2008, 3:22.
doi: 10.1186/1750-1172-3-22 pmid: 18667063 |
| [6] |
LI N, GU H F. Genetic and biological effects of SLC12A3, a sodium-chloride cotransporter, in gitelman syndrome and diabetic kidney disease[J]. Front Genet, 2022, 13:799224.
doi: 10.3389/fgene.2022.799224 URL |
| [7] | GITELMAN综合征诊治专家共识协作组. Gitelman综合征诊治专家共识[J]. 中华内科杂志, 2017, 56(9):712-716. |
| Gitelman Syndrome Collaboratwe Study Group. Expert consensus for the diagnosis and treatment of patients with Gitelman syndrome[J]. Chin J Intern Med, 2017, 56(9):712-716. | |
| [8] | 马骏, 任红, 谢静远, 等. Gitelman综合征47例临床特征分析[J]. 中国实用内科杂志, 2014, 34(3):273-276,280. |
| MA J, REN H, XIE J Y, et al. Clinical features of patients with Gitelman syndrome[J]. Chin J Pract Intern Med, 2014, 34(3):273-276,280. | |
| [9] |
CABRAL B M I, EDDING S N, PORTOCARRERO J P, et al. Rhabdomyolysis[J]. Dis Mon, 2020, 66(8):101015.
doi: 10.1016/j.disamonth.2020.101015 URL |
| [10] | SAURET J M, MARINIDES G, WANG G K. Rhabdo-myolysis[J]. Am Fam Physician, 2002, 65(5):907-912. |
| [11] |
ZIMMERMAN J L, SHEN M C. Rhabdomyolysis[J]. Chest, 2013, 144(3):1058-1065.
doi: S0012-3692(13)60626-1 pmid: 24008958 |
| [12] |
HE R, GUO W J, SHE F, et al. A rare case of hypokalemia-induced rhabdomyolysis[J]. J Geriatr Cardiol, 2018, 15(4):321-324.
doi: 10.4067/S0034-98872014000500015 URL |
| [13] | [ LUZARDO L, SILVARIÑO R, BOGGIA J, et al. Severe hypokalemic rhabdomyolysis. Report of six cases[J]. Rev Med Chil, 2014, 142(5):651-655. |
| [14] | PECNIK P, MÜLLER P, VRABEL S, et al. Two cases of hypokalaemic rhabdomyolysis: same but different[J]. BMJ Case Rep, 2018, 2018:bcr2017223609. |
| [15] |
VON VIGIER R O, ORTISI M T, LA MANNA A, et al. Hypokalemic rhabdomyolysis in congenital tubular disorders: a case series and a systematic review[J]. Pediatr Nephrol, 2010, 25(5):861-866.
doi: 10.1007/s00467-009-1388-2 pmid: 20033223 |
| [16] |
NISHIHARA G, HIGASHI H, MATSUO S, et al. Acute renal failure due to hypokalemic rhabdomyolysis in Gitelman's syndrome[J]. Clin Nephrol, 1998, 50(5):330-332.
pmid: 9840323 |
| [17] |
KUMAGAI H, MATSUMOTO S, NOZU K. Hypokalemic rhabdomyolysis in a child with Gitelman's syndrome[J]. Pediatr Nephrol, 2010, 25(5):953-955.
doi: 10.1007/s00467-009-1412-6 pmid: 20072789 |
| [18] |
YANG L Y, YIN J H, YANG J, et al. Liquorice-induced severe hypokalemic rhabdomyolysis with Gitelman syndrome and diabetes: a case report[J]. World J Clin Cases, 2019, 7(10):1200-1205.
doi: 10.12998/wjcc.v7.i10.1200 URL |
| [19] |
XU J, HE J, XU S, et al. Gitelman syndrome with Graves' disease leading to rhabdomyolysis: a case report and lite-rature review[J]. BMC Nephrol, 2023, 24(1):123.
doi: 10.1186/s12882-023-03180-8 |
| [20] |
MA J, REN H, LIN L, et al. Genetic features of Chinese patients with Gitelman syndrome: sixteen novel SLC12A3 mutations identified in a New Cohort[J]. Am J Nephrol, 2016, 44(2):113-121.
doi: 10.1159/000447366 URL |
| [21] |
LIU S, KE J, ZHANG B, et al. A novel compound heterozygous variant of SLC12A3 gene in a pedigree with Gitelman syndrome co-existent with thyroid dysfunction[J]. Endocr Pract, 2018, 24(10):889-893.
doi: 10.4158/EP-2018-0218 URL |
| [22] | FUJIMURA J, NOZU K, YAMAMURA T, et al. Clinical and genetic characteristics in patients with Gitelman syndrome[J]. Kidney Int Rep, 2018, 4(1):119-125. |
| [23] |
MIZOKAMI T, HISHINUMA A, KOGAI T, et al. Graves' disease and Gitelman syndrome[J]. Clin Endocrinol (Oxf), 2016, 84(1):149-150.
doi: 10.1111/cen.12829 URL |
| [24] |
CHANDRA A K, GOSWAMI H, SENGUPTA P. Effects of magnesium on cytomorphology and enzyme activities in thyroid of rats[J]. Indian J Exp Biol, 2014, 52(8):787-792.
pmid: 25141541 |
| [25] |
MONCAYO R, MONCAYO H. The WOMED model of benign thyroid disease: Acquired magnesium deficiency due to physical and psychological stressors relates to dysfunction of oxidative phosphorylation[J]. BBA Clin, 2014, 3:44-64.
doi: 10.1016/j.bbacli.2014.11.002 URL |
| [26] | 周文华, 杨爱华, 牟利军. 四例Gitelman综合征继发横纹肌溶解综合征报告[J]. 中华急诊医学杂志, 2021, 30(4):500-503. |
| ZHOU W H, YANG A H, MOU L J. Four cases of Stria-ted muscle tissue lysis syndrome secondary to Gitelman syndrome[J]. Chin J Emerg Med, 2021, 30(4):500-503. | |
| [27] | 石凯丽, 杜东海, 韩虹, 等. 儿童Gitelman综合征合并横纹肌溶解症一例并文献复习[J]. 中国药物与临床, 2019, 19(11):1886-1887. |
| SHI K L, DU D H, HAN H, et al. A case of Gitelman syndrome with Rhabdomyolysis in children and literature review[J]. Chin Remedies Clin, 2019, 19(11):1886-1887. | |
| [28] | 彭稚媚, 莫南凤, 马明明, 等. Gitelman综合征纯合变异合并重度低钾血症一例[J]. 海南医学, 2019, 30(18):2437-2439. |
| PENG Z M, MO N F, MA M M, et al. A case of homozygous variation with severe hypokalemia in Gitelman syndrome[J]. Hainan Med J, 2019, 30(18):2437-2439. | |
| [29] |
HUANG C L, KUO E. Mechanism of hypokalemia in magnesium deficiency[J]. J Am Soc Nephrol, 2007, 18(10):2649-2652.
doi: 10.1681/ASN.2007070792 URL |
| [1] | 丁秋兰, 王学锋. 遗传性易栓症的表型和基因诊断流程[J]. 诊断学理论与实践, 2019, 18(2): 127-132. |
| [2] | 陈乐, 黄婷, 谢梦琦, 陆文丽, 马晓宇, 王歆琼, 许春娣, 李卫,. 幼年型粒单核细胞白血病2例报道及文献复习[J]. 诊断学理论与实践, 2015, 14(03): 235-238. |
| [3] | 刘淑平, 丁洁, 姚勇, 俞礼霞, 王芳,. 儿童Gitelman综合征一例并文献复习[J]. 诊断学理论与实践, 2014, 13(05): 524-528. |
| [4] | 余永国,. 染色体基因芯片分析技术在不明原因智力落后诊断中的应用——附500例基因芯片结果分析[J]. 诊断学理论与实践, 2013, 12(04): 387-389. |
| [5] | 王伟,. 遗传性代谢疾病的临床检测与基因诊断[J]. 诊断学理论与实践, 2013, 12(04): 401-405. |
| [6] | 吕建新, 张杰,. 线粒体遗传性疾病的基因诊断[J]. 诊断学理论与实践, 2013, 12(04): 381-386. |
| [7] | 李春光, 李志刚, 陈和忠, 苏长青,. 食管癌诊断治疗的重要靶标Survivin[J]. 诊断学理论与实践, 2011, 10(06): 571-574. |
| [8] | 顾鸣敏,. 人类遗传性疾病基因诊断的回顾与展望[J]. 诊断学理论与实践, 2010, 9(05): 420-423. |
| [9] | 李磊, 杨涛, 吴皓,. 耳聋基因的筛查与诊断[J]. 诊断学理论与实践, 2010, 9(05): 409-412. |
| [10] | 陆晔玲, 丁秋兰, 戴菁, 谢炳寿, 王明山, 奚晓东, 王鸿利, 王学锋,. 同时存在血友病A及血友病B患者家系的基因诊断[J]. 诊断学理论与实践, 2010, 9(05): 443-448. |
| [11] | . 更正说明[J]. 诊断学理论与实践, 2009, 8(04): 462-. |
| [12] | 陆晔玲, 丁秋兰, 戴菁, 王鸿利, 奚晓东, 王学锋,. FⅧ基因内含子1倒位及X染色体非随机灭活导致的女性血友病A1例[J]. 诊断学理论与实践, 2008, 7(03): 286-290. |
| [13] | 宁光. 重视内分泌代谢病的基因检测[J]. 诊断学理论与实践, 2003, 2(02): 5-6. |
| [14] | 胡敏. 营养不良性心脏钙化基因诊断的研究进展[J]. 诊断学理论与实践, 2002, 1(04): 66-67. |
| [15] | 丁培芳. 血友病A基因诊断和产前诊断技术的研究进展[J]. 诊断学理论与实践, 2002, 1(02): 60-62. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||