诊断学理论与实践 ›› 2022, Vol. 21 ›› Issue (03): 343-348.doi: 10.16150/j.1671-2870.2022.03.009
徐琛莹a, 李嫣然a, 倪晓枫b, 徐上妍b, 林青a( )
)
收稿日期:2022-05-19
出版日期:2022-06-25
发布日期:2022-08-17
通讯作者:
林青
E-mail:lq11035@rjh.com.cn
XU Chenyinga, LI Yanrana, NI Xiaofengb, XU Shangyanb, LIN Qinga()
Received:2022-05-19
Online:2022-06-25
Published:2022-08-17
Contact:
LIN Qing
E-mail:lq11035@rjh.com.cn
摘要:
目的:分析超声预测老年甲状腺乳头状癌(papillary thyroid carcinomas, PTC)的颈部淋巴结转移效能及相关超声影像特征。方法:回顾分析2021年1月至2021年10月上海交通大学医学院附属瑞金医院收治的232例PTC老年患者(≥60岁)术前的超声图像特征,并根据其术后病理提示有无颈部淋巴结转移,分为转移组与非转移组。计算超声诊断PTC颈部淋巴结转移的效能,采用因素分析颈部淋巴结转移的超声征像,采用Logistic回归模型分析提示PTC颈部淋巴结转移的原发灶超声征像,并构建多因素模型,利用受试者操作特征(receiver operator characteristic,ROC)曲线评价危险因素模型预测PTC颈部淋巴结转移的价值。结果:232例PTC老年患者中,30.6%的患者(71例)术后病理示存在颈部淋巴结转移。超声诊断PTC颈部淋巴结转移的灵敏度为40.8%(29/232),特异度为93.2%(150/232),阳性预测值为72.5%(29/40),阴性预测值为78.1%(150/192)。单因素分析示,术前超声征象中,原发灶结节大小≥10 mm、微钙化、紧贴包膜及彩色多普勒血流显像(color Doppler flow imaging,CDFI)示血流丰富的患者颈部淋巴结转移率较高(P<0.05)。多因素分析示,术前超声影像示原发灶结节大小≥10 mm[优势比(odd ratio,OR)=4.093,95%置信区间(confidence interval,CI)为1.933~8.666,P<0.001]及紧贴包膜(OR=2.177,95%CI为1.101~4.302,P=0.025)是颈部淋巴结转移的独立危险因素;二者同时存在诊断PTC颈部淋巴结转移的曲线下面积(area under the value,AUC)为0.709,较单个征象诊断的AUC大(紧贴包膜的AUC为0.602;结节大小≥10 mm的AUC为0.668)。结论:在老年PTC患者中,淋巴结转移者约占30.6%,术前超声征象中的原发灶结节大小≥10 mm、紧贴包膜是肿瘤发生颈部淋巴结转移的独立危险因素。
中图分类号:
徐琛莹, 李嫣然, 倪晓枫, 徐上妍, 林青. 超声预测老年甲状腺乳头状癌患者颈部淋巴结转移的效能及相关超声征象分析[J]. 诊断学理论与实践, 2022, 21(03): 343-348.
XU Chenying, LI Yanran, NI Xiaofeng, XU Shangyan, LIN Qing. Efficacy of ultrasonic examination in predicting cervical lymph node metastasis in elderly patients with papillary thyroid carcinoma and analysis of related ultrasound signs[J]. Journal of Diagnostics Concepts & Practice, 2022, 21(03): 343-348.
表1
老年PTC患者颈部淋巴结转移的术前一般临床及超声资料分析[例(%)]
| 临床特征 | 总数(n=232) | 颈部淋巴结转移[例(%)] | P值 | |
|---|---|---|---|---|
| 有(n=71) | 无(n=161) | |||
| 年龄(岁) | 65.06±3.94 | 64.65±3.91 | 65.24±3.95 | 0.290 |
| 60~69 | 199(85.9%) | 62(87.3%) | 137(85.1%) | 0.654 |
| ≥70 | 33(14.2%) | 9(12.7%) | 24(14.9%) | |
| 性别 | 0.980 | |||
| 男 | 39(16.8%) | 12(16.9%) | 27(16.8%) | |
| 女 | 193(83.2%) | 59(83.1%) | 134(83.2%) | |
| BMI(kg/m2) | 24.39±3.26 | 24.56±3.26 | 24.32±3.27 | 0.599 |
| 恶性肿瘤家族史 | 0.427 | |||
| 有 | 18(7.8%) | 7(9.9%) | 11(6.8%) | |
| 无 | 214(92.2%) | 64(90.1%) | 150(93.2%) | |
| 结节部位 | 0.052 | |||
| 单侧 | 173(74.6%) | 47(66.2%) | 126(78.3%) | |
| 多侧 | 59(25.4%) | 24(33.8%) | 35(21.7%) | |
| 结节个数 | 0.155 | |||
| 单个 | 162(70.3%) | 45(63.4%) | 117(72.7%) | |
| 多个 | 70(29.7%) | 26(36.6%) | 44(27.3%) | |
| 结节大小 (mm) | 10.01±6.92 | 13.40±8.74 | 8.52±5.33 | <0.001 |
| <10 | 152(65.5%) | 30(42.3%) | 122(75.8%) | <0.001 |
| ≥10 | 80(34.5%) | 41(57.7%) | 39(24.2%) | |
| 结节方位 | 0.063 | |||
| 垂直 | 151(65.1%) | 40(56.3%) | 111(68.9%) | |
| 水平 | 81(34.9%) | 31(43.7%) | 50(31.1%) | |
| 结节内部结构 | 0.578 | |||
| 实性 | 223(96.1%) | 69(97.2%) | 154(95.7%) | |
| 非实性 | 9(3.9%) | 2(2.8%) | 7(4.3%) | |
| 结节内部回声 | 0.220 | |||
| 极低回声 | 13(5.6%) | 2(2.8%) | 11(6.8%) | |
| 非极低回声 | 219(94.4%) | 69(97.2%) | 150(93.2%) | |
| 结节边缘 | 0.281 | |||
| 不规则 | 197(84.9%) | 63(88.7%) | 134(83.2%) | |
| 规则 | 35(15.1%) | 8(11.3%) | 27(16.8%) | |
| 微钙化 | 0.022 | |||
| 有 | 141(60.8%) | 51(71.8%) | 90(55.9%) | |
| 无 | 91(39.2%) | 20(28.2%) | 71(44.1%) | |
| 慧星尾征 | 1.000 | |||
| 有 | 0(0) | 0(0) | 0(0) | |
| 无 | 232(100%) | 71(30.6%) | 161(69.4%) | |
| CDFI血流 | 0.004 | |||
| 丰富 | 25(10.8%) | 14(19.7%) | 11(6.8%) | |
| 非丰富 | 207(89.2%) | 57(80.3%) | 150(93.2%) | |
| 紧贴包膜 | 0.004 | |||
| 有 | 111(47.8%) | 44(62.0%) | 67(41.6%) | |
| 无 | 121(52.2%) | 27(38.0%) | 94(58.4%) | |
| C-TIRADS分类 | 0.089 | |||
| 3 | 1(0.4%) | 0(0) | 1(0.4%) | |
| 4A | 6(2.6%) | 3(4.2%) | 3(1.9%) | |
| 4B | 47(20.3%) | 8(11.3%) | 39(24.2%) | |
| 4C | 173(74.6%) | 59(83.1%) | 114(70.8%) | |
| 5 | 5(2.2%) | 1(1.4%) | 4(2.5%) | |
表2
老年PTC癌患者颈部淋巴结转移的Logistic多因素回归分析
| 自变量 | OR | 95%CI | P值 |
|---|---|---|---|
| 性别 | 0.287~1.726 | 0.443 | |
| 女 | 1.00 | ||
| 男 | 0.704 | ||
| 年龄(岁) | 0.313~1.906 | 0.576 | |
| 60~69 | 1.00 | ||
| ≥70 | 0.773 | ||
| 结节部位 | 0.510~15.905 | 0.233 | |
| 单侧 | 1.00 | ||
| 多侧 | 2.847 | ||
| 结节个数 | 0.082~2.365 | 0.339 | |
| 单个 | 1.00 | ||
| 多个 | 0.441 | ||
| 结节大小(mm) | 1.933~8.666 | <0.001 | |
| <10 | 1.00 | ||
| ≥10 | 4.093 | ||
| 方向 | 0.358~1.938 | 0.671 | |
| 水平 | 1.00 | ||
| 垂直 | 0.833 | ||
| 边缘 | 0.163~1.725 | 0.292 | |
| 规则 | 1.00 | ||
| 不规则 | 0.531 | ||
| 内部结构 | 0.162~7.114 | 0.942 | |
| 非实性 | 1.00 | ||
| 实性 | 1.073 | ||
| 内部回声 | 0.056~1.440 | 0.128 | |
| 非极低回声 | 1.00 | ||
| 极低回声 | 0.283 | ||
| 微钙化 | 0.366~1.969 | 0.703 | |
| 无 | 1.00 | ||
| 有 | 0.849 | ||
| 紧贴包膜 | 1.101~4.302 | 0.025 | |
| 无 | 1.00 | ||
| 有 | 2.177 | ||
| CDFI血流信号 | 0.779~5.769 | 0.141 | |
| 非丰富 | 1.00 | ||
| 丰富 | 2.120 | ||
| C-TIRADS分类 | 0.937~13.813 | 0.062 | |
| 3~4B | 1.00 | ||
| 4C~5 | 3.598 |
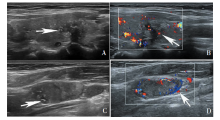
图1
左侧PTC伴颈部淋巴结转移的超声声像图 女,61岁,超声见左侧甲状腺内结节,C-TIRADS 4C类。左侧颈部见异常淋巴结。A:左侧甲状腺内见一个结节,大小16.7 mm×8.3 mm×8.8 mm,内部呈实性低回声,水平位生长,紧贴背外侧包膜,边缘不规则,见散在微钙化(箭头);B:CDFI显示,结节内部及周边见少许血流信号(箭头);C:左侧颈部Ⅲ区可见大小27.0 mm×11.5 mm×16.9 mm的淋巴结,淋巴门未见,内部呈高回声,见微钙化(箭头);D:CDFI显示,淋巴结周边见较丰富血流信号(箭头)。
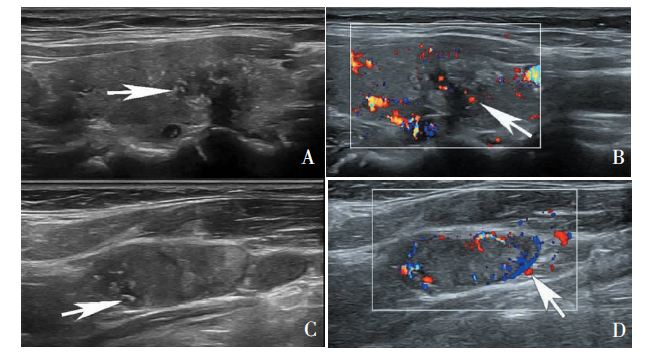
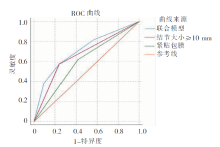
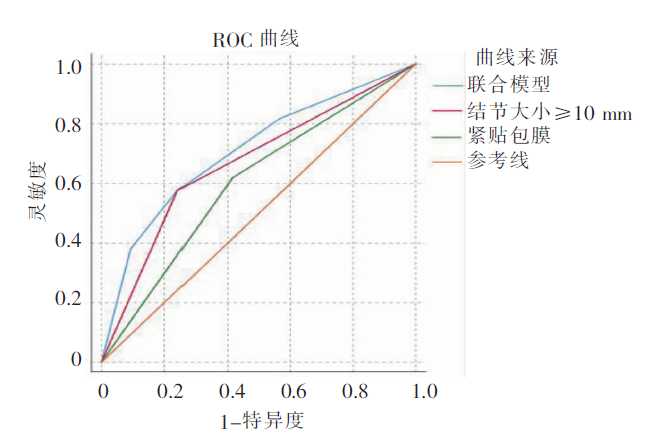
图2
多因素Logistic回归模型ROC曲线图
| [1] |
Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2021, 71(3):209-249.
doi: 10.3322/caac.21660 URL |
| [2] | Xia C, Dong X, Li H, et al. Cancer statistics in China and United States, 2022: profiles, trends, and determinants[J]. Chin Med J (Engl), 2022, 135(5):584-590. |
| [3] | 杨雷, 王宁. 甲状腺癌流行病学研究进展[J]. 中华预防医学杂志, 2014, 48(8):744-748. |
| Yang L, Wang N. Thyroid cancer epidemiolog, reviem[J]. Chin J Prev Med, 2014, 48(8):744-748. | |
| [4] |
Gambardella C, Tartaglia E, Nunziata A, et al. Clinical significance of prophylactic central compartment neck dissection in the treatment of clinically node-negative papillary thyroid cancer patients[J]. World J Surg Oncol, 2016, 14(1):247.
doi: 10.1186/s12957-016-1003-5 pmid: 27644091 |
| [5] |
Zaydfudim V, Feurer ID, Griffin MR, et al. The impact of lymph node involvement on survival in patients with papil-lary and follicular thyroid carcinoma[J]. Surgery, 2008, 144(6):1070-1077.
doi: 10.1016/j.surg.2008.08.034 URL |
| [6] |
Davies L, Welch HG. Increasing incidence of thyroid cancer in the United States, 1973-2002[J]. Jama, 2006, 295(18):2164-2167.
doi: 10.1001/jama.295.18.2164 URL |
| [7] | 张伟红, 闫红莲, 魏云, 等. 超声检查诊断甲状腺癌合并淋巴结转移的临床研究[J]. 实用癌症杂志, 2021, 36(6):954-958. |
| Zhang WH, Yan HL, Wei Y, et al. Clinical research on ultrasonic examination in the diagnosis of thyroid cancer combined with lymph node metastasis[J]. The Pract J Cancer, 2021, 36(6):954-958. | |
| [8] |
Kuna SK, Bracic I, Tesic V, et al. Ultrasonographic differentiation of benign from malignant neck lymphadenopathy in thyroid cancer[J]. J Ultrasound Med, 2006, 25(12):1531-1537.
doi: 10.7863/jum.2006.25.12.1531 URL |
| [9] |
Leenhardt L, Erdogan MF, Hegedus L, et al. 2013 European thyroid association guidelines for cervical ultrasound scan and ultrasound-guided techniques in the postoperative management of patients with thyroid cancer[J]. Eur Thyroid J, 2013, 2(3):147-159.
doi: 10.1159/000354537 pmid: 24847448 |
| [10] |
杨雷, 郑荣寿, 王宁, 等. 2013年中国甲状腺癌发病与死亡情况[J]. 中华肿瘤杂志, 2017, 39(11):862-867.
pmid: 29151294 |
|
Yang L, Zheng RS, Wang N, et al. Analysis of incidence and mortality of thyroid cancer in China,2013[J]. Chin J Oncol, 2017, 39(11):862-867.
doi: 10.3760/cma.j.issn.0253-3766.2017.11.010 pmid: 29151294 |
|
| [11] |
Edafe O, Wadsley J, Harrison BJ, et al. Treatment related morbidity in differentiated thyroid cancer-a survey of clinicians[J]. Thyroid Res, 2014, 7(1):3.
doi: 10.1186/1756-6614-7-3 pmid: 24618295 |
| [12] |
Sosa JA, Hanna JW, Robinson KA, et al. Increases in thyroid nodule fine-needle aspirations, operations, and diagnoses of thyroid cancer in the United States[J]. Surgery, 2013, 154(6):1420-1426.
doi: 10.1016/j.surg.2013.07.006 URL |
| [13] |
Peterson E, De P, Nuttall R. BMI, diet and female reproductive factors as risks for thyroid cancer: a systematic review[J]. PLoS One, 2012, 7(1):e29177.
doi: 10.1371/journal.pone.0029177 URL |
| [14] |
Conzo G, Avenia N, Bellastella G, et al. The role of surgery in the current management of differentiated thyroid cancer[J]. Endocrine, 2014, 47(2):380-388.
doi: 10.1007/s12020-014-0251-9 URL |
| [15] |
Liu C, Xiao C, Chen J, et al. Risk factor analysis for predicting cervical lymph node metastasis in papillary thyroid carcinoma: a study of 966 patients[J]. BMC Cancer, 2019, 19(1):622.
doi: 10.1186/s12885-019-5835-6 URL |
| [16] |
Ahn BH, Kim JR, Jeong HC, et al. Predictive factors of central lymph node metastasis in papillary thyroid carcinoma[J]. Ann Surg Treat Res, 2015, 88(2):63-68.
doi: 10.4174/astr.2015.88.2.63 URL |
| [17] |
Shah Y, Verma A, Marderstein AR, et al. Pan-cancer analysis reveals molecular patterns associated with age[J]. Cell Rep, 2021, 37(10):110100.
doi: 10.1016/j.celrep.2021.110100 URL |
| [18] |
Attard A, Paladino NC, Lo Monte AI, et al. Skip metastases to lateral cervical lymph nodes in differentiated thyroid cancer: a systematic review[J]. BMC Surg, 2019, 18(Suppl 1):112.
doi: 10.1186/s12893-018-0435-y URL |
| [19] |
Xu JM, Xu HX, Li XL, et al. A risk model for predicting central lymph node metastasis of papillary thyroid microcarcinoma including conventional ultrasound and acoustic radiation force impulse elastography[J]. Medicine (Baltimore), 2016, 95(3):e2558.
doi: 10.1097/MD.0000000000002558 URL |
| [20] | Liu Z, Wang L, Yi P, et al. Risk factors for central lymph node metastasis of patients with papillary thyroid microcarcinoma: a meta-analysis[J]. Int J Clin Exp Pathol, 2014, 7(3):932-7. |
| [21] |
Mazzaferri EL. Management of low-risk differentiated thyroid cancer[J]. Endocr Pract, 2007, 13(5):498-512.
doi: 10.4158/EP.13.5.498 pmid: 17872353 |
| [22] |
Ito Y, Miyauchi A, Inoue H, et al. An observational trial for papillary thyroid microcarcinoma in Japanese patients[J]. World J Surg, 2010, 34(1):28-35.
doi: 10.1007/s00268-009-0303-0 URL |
| [23] |
Kim JW, Roh JL, Gong G, et al. Extent of extrathyroidal extension as a significant predictor of nodal metastasis and extranodal extension in patients with papillary thyroid carcinoma[J]. Ann Surg Oncol, 2017, 24(2):460-468.
doi: 10.1245/s10434-016-5594-4 URL |
| [24] |
Kamaya A, Tahvildari AM, Patel BN, et al. Sonographic detection of extracapsular extension in papillary thyroid cancer[J]. J Ultrasound Med, 2015, 34(12):2225-2230.
doi: 10.7863/ultra.15.02006 pmid: 26518279 |
| [25] |
Zhou J, Yin L, Wei X, et al. 2020 Chinese guidelines for ultrasound malignancy risk stratification of thyroid nodu-les: the C-TIRADS[J]. Endocrine, 2020, 70(2):256-279.
doi: 10.1007/s12020-020-02441-y URL |
| [1] | 王文涵, 夏蜀珺, 詹维伟. 长链非编码RNA ENST00000489676在超声评估甲状腺乳头状癌颈部淋巴结转移中的应用[J]. 诊断学理论与实践, 2022, 21(04): 514-519. |
| [2] | 张红, 朱梦梦. 新型冠状病毒肺炎疫情期间老年人进食安全护理[J]. 诊断学理论与实践, 2022, 21(02): 277-280. |
| [3] | 丁燕飞, 陈平, 罗方秀, 吴云林. 以左锁骨上淋巴结肿大为首发表现的结肠癌一例报道[J]. 诊断学理论与实践, 2021, 20(06): 584-587. |
| [4] | 何碧媛, 周毓青, 姚秉彝, 曹力, 包丽. 中孕期弹性超声成像宫颈机能智能定量分析预测自发性早产的临床应用价值[J]. 诊断学理论与实践, 2021, 20(05): 450-455. |
| [5] | 刘安平, 凌枫, 史超, 孙璟. 上海社区老年脑卒中患者跌倒风险因素分析及风险识别模型的建立[J]. 诊断学理论与实践, 2021, 20(05): 475-479. |
| [6] | 况李君, 陶玲玲, 詹维伟, 李伟伟, 樊金芳, 周伟. 负压细针抽吸和毛细抽吸活检法穿刺洗脱液中甲状腺球蛋白测定在甲状腺乳头状癌淋巴结转移中的诊断价值比较[J]. 诊断学理论与实践, 2021, 20(04): 367-371. |
| [7] | 杨一娴, 倪仲馨, 夏蜀珺, 周伟, 詹维伟. 多灶性与单灶性甲状腺乳头状癌的临床病理特征及超声表现的比较[J]. 诊断学理论与实践, 2021, 20(02): 168-172. |
| [8] | 吴洁, 冯媛媛, 任妍, 曹久妹. 基于冠状动脉造影检查的高龄老年人群发生冠心病的危险因素调查及相应诊断模型的建立[J]. 诊断学理论与实践, 2021, 20(02): 201-206. |
| [9] | 周伟, 陈易来, 詹维伟. 细针穿刺洗脱液中甲状腺球蛋白检测在诊断分化型甲状腺癌淋巴结转移中的应用进展[J]. 诊断学理论与实践, 2020, 19(04): 339-343. |
| [10] | 王星, 汪蓉晖, 张桂萍, 董屹婕, 周伟, 詹维伟. 10 388个甲状腺结节行超声引导下细针抽吸活检的甲状腺癌各亚型诊断准确率的10年研究[J]. 诊断学理论与实践, 2020, 19(04): 359-363. |
| [11] | 闫冰, 王海飞, 曹云云, 牛建梅. 乳腺黏液腺癌超声声像图特征与临床病理分型的对照及误诊分析[J]. 诊断学理论与实践, 2020, 19(04): 386-390. |
| [12] | 洪贵平, 陈晓炎, 周剑平, 陈巍, 项轶, 周敏, 李庆云. 超声引导下经支气管针吸活检在老年患者肺门及纵隔病变中的诊断价值及漏诊分析[J]. 诊断学理论与实践, 2020, 19(04): 397-401. |
| [13] | 周郁芬, 王柏凯, 罗芳秀, 徐莹, 丁燕飞, 袁晓琴, 陈平, 吴云林. 上海地区36 857例胃镜胃息肉检出率及临床特征分析[J]. 诊断学理论与实践, 2020, 19(04): 420-425. |
| [14] | 王燕, 张静雯, 詹维伟. 高频超声检查联合动态试验诊断咽食管憩室的价值[J]. 诊断学理论与实践, 2020, 19(03): 264-268. |
| [15] | 郭艳, 葛娟娟, 陈晨, 尹吉明, 王小龙, 陈家庚, 杜燕伟, 段园园, 凡雪霖, 郑磊, 王西勇, 詹维伟, 张璐. 细针穿刺活检联合RJ-TIRADS在诊断老年甲状腺结节良恶性中的价值[J]. 诊断学理论与实践, 2020, 19(03): 286-291. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||