诊断学理论与实践 ›› 2023, Vol. 22 ›› Issue (02): 127-133.doi: 10.16150/j.1671-2870.2023.02.004
郝家琪1,2, 王鑫鹭1, 胡晓帆1, 潘晓霞1, 徐静1( ), 马骏1()
), 马骏1()
收稿日期:2023-02-16
出版日期:2023-04-25
发布日期:2023-08-31
通讯作者:
马骏 E-mail: jiangpuma@163.com; 徐静 E-mail:xj11564@rjh.com.cn
基金资助:
HAO Jiaqi1,2, WANG Xinlu1, HU Xiaofan1, PAN Xiaoxia1, XU Jing1(), MA Jun1()
Received:2023-02-16
Online:2023-04-25
Published:2023-08-31
摘要:
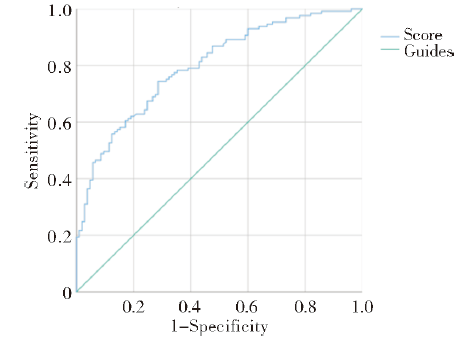
目的:分析急性肾小管间质性肾炎(acute tubulointerstitial nephritis, ATIN)患者的临床及实验室检查特征,探讨该病与急性肾小管坏死(acute tubular necrosis nephritis, ATN)的鉴别诊断要点。方法:纳入2009年1月至2018年12月间在上海交通大学医学院附属瑞金医院肾脏科经肾活检病理诊断为ATIN、ATN的患者,收集其临床表现和实验室检查数据,并对两者进行比较分析。结果:10年间我院肾脏科行经肾活检的病例总计5 537例,其中诊断为ATIN的患者共135例(2.4%,135/5 537),诊断为ATN的患者109例(2.0%,109/5 537)。ATIN占急性肾脏病(acute kidney disease, AKD)肾活检患者的21.4%(135/630)。ATIN患者的中位确诊年龄为53岁,女性占57.0%,临床主要表现为发热、皮疹、关节痛,常见诱因为感染、药物应用和毒物接触。与ATN组相比,ATIN患者中女性占比高(57.0%比33.9%),平均体重指数(body weight index,BMI)低(22.9±3.6比24.6±3.9,P<0.01),且发生急性肾损伤(acute kidney injury, AKI)(14.8% 比64.2%)、少尿(17.0%比48.6%)及入院后需紧急透析(19.3%比39.4%)的百分比低(P<0.01)。ATIN患者入院时,血红蛋白(hemoglobin,Hb)[(100.9±20.9) g/L比(116.7±29.8) g/L]和血尿素氮/肌酐比值(blood urea nitrogen/creatinine ratio, BCR)(11.8±5.4比14.6±11.0)均较ATN组低(P<0.01)。多因素回归分析显示,入院时高白蛋白(>55 g/L)、低血清肌酐(serum creatine,Scr)(<62 μmol/L)、低血清尿酸(urine acid,UA)(<208 μmol/L)、低Hb水平(<130 g/L)与ATIN相关,联合这4项指标建立的预测模型,其诊断ATIN的受试者操作特征曲线下面积为0.798(95%CI为0.742~0.853),灵敏度为74.4%,特异度为71.4%。结论:ATIN在上海地区人群接受肾活检的AKD患者中占比高,好发于中年女性,半数患者诱因不明。患者入院时的白蛋白、Scr、Hb及UA水平有助于ATIN与AIN间的鉴别,基于上述4项指标构建的ATIN患者诊断预测模型具有较好的特异度和灵敏度。
中图分类号:
郝家琪, 王鑫鹭, 胡晓帆, 潘晓霞, 徐静, 马骏. 急性肾小管间质性肾炎与急性肾小管坏死的临床鉴别分析[J]. 诊断学理论与实践, 2023, 22(02): 127-133.
HAO Jiaqi, WANG Xinlu, HU Xiaofan, PAN Xiaoxia, XU Jing, MA Jun. Clinical differential diagnosis of acute tubulointerstitial nephritis and acute tubular necrosis[J]. Journal of Diagnostics Concepts & Practice, 2023, 22(02): 127-133.
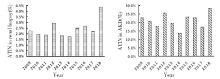
图1
ATIN在肾活检和AKD中的占比
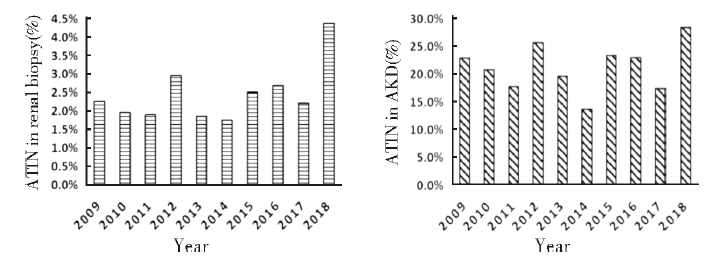
表1
ATN与ATIN患者的临床资料比较
| Indice | ATN(n=109) | ATIN(n=135) | P |
|---|---|---|---|
| Male(%) | 72(66.1%) | 58(43.0%) | <0.01 |
| Age(year) | 49(15-85) | 53(14-82) | 0.09 |
| BMI(kg/m2) | 24.6±3.9 | 22.9±3.6 | <0.01 |
| AKD disease course(%) | 82(75.2%) | 60(44.4%) | <0.01 |
| AKI(%) | 70(64.2%) | 20(14.8%) | <0.01 |
| Urgent dialysis needed during hospitalization (%) | 43(39.4%) | 26(19.3%) | <0.01 |
| Dialysis independent at hospital discharge(%) | 22(51.2%) | 20(76.9%) | 0.03 |
| Clinical manifestation | |||
| Fever(%) | 23(21.1%) | 40(29.6%) | 0.12 |
| Rash(%) | 9(8.3%) | 10(7.4%) | 0.08 |
| Arthralgia(%) | 6(5.5%) | 4(3.0%) | 0.32 |
| Oliguria(%) | 53(48.6%) | 23(17.0%) | <0.01 |
| Inducement | |||
| Infection(%) | 22(20.2%) | 31(23.0%) | 0.60 |
| Toxicant(%) | 8(7.3%) | 2(1.5%) | 0.05 |
| Drugs(%) | 30(27.5%) | 34(25.2%) | 0.68 |
| Unknown(%) | 49(45.0%) | 68(50.4%) | 0.40 |
| Hypertension(%) | 39(35.8%) | 52(38.5%) | 0.66 |
| Diabetes(%) | 8(7.3%) | 11(8.1%) | 0.82 |
表2
ATN和ATIN患者的实验室检查结果比较
| Indice | ATN(n=109) | ATIN(n=135) | P |
|---|---|---|---|
| Scr at admission(μmol/L) | 314(81-2 290) | 238(101-876) | <0.01 |
| Peak Scr (μmol/L) | 425(102-2 290) | 278(115-1 270) | <0.01 |
| Scr at discharge(μmol/L) | 264(54-1 059) | 171.5(50-876) | 0.66 |
| Prealbumin(mg/L) | 225.1±78.7 | 225.1±61.6 | 1.00 |
| Alb(g/L) | 26(8-46) | 34(12-43) | <0.01 |
| Uric acid(μmol/L) | 454(149-874) | 345(104-779) | <0.01 |
| TG(mmol/L) | 2.1(0.8-15.1) | 1.7(0.5-7.0) | <0.01 |
| TC(mmol/L) | 5.1(0.9-21.8) | 4.4(1.6-19.8) | <0.01 |
| PTH(pg/mL)* | 1.9±0.4 | 1.9±0.4 | 0.30 |
| Hb(g/L) | 116.7±29.8 | 100.9±20.9 | <0.01 |
| BCR | 14.6±11.0 | 11.8±5.4 | 0.02 |
| 24 h urine protein(mg/24 h) | 1 350(52-23 555) | 1 036(75-27 303) | 0.31 |
| hematuria(%) | 0.54 | ||
| Gross hematuria(%) | 11(10.1%) | 12(8.9%) | |
| Microscopic hematuria(%) | 41(37.6%) | 43(31.9%) | |
| Urinary sodium/Potassium ratio | 2.2(0.1-15.8) | 2.8(0.2-21.5) | 0.04 |
| Urinary urea nitrogen (mmol/24 h)# | 12.9±4.2 | 12.6±4.4 | 0.57 |
表3
ATIN的危险因素分析
| Indice | Single factor regression | Multiple regression | |||
|---|---|---|---|---|---|
| OR(95%CI) | P | OR(95%CI) | P | ||
| Clinical data | |||||
| Female(%) | 2.58(1.53-4.36) | <0.01 | - | - | |
| Age(year) | 1.01(1.00-1.03) | 0.07 | - | - | |
| Non-AKI | 10.3(5.58-19.1) | <0.01 | - | - | |
| Non-oliguria | 4.61(2.57-8.27) | <0.01 | - | - | |
| BMI | 0.88(0.82-0.96) | <0.01 | - | - | |
| Treatment | |||||
| Urgent dialysis unneeded during hospitalization | 2.73(1.54-4.85) | <0.01 | - | - | |
| Dialysis independent at hospital discharge | 3.18(1.07-9.47) | 0.04 | - | - | |
| Laboratory examination | |||||
| Scr at admission(μmol/L) | 0.998(0.997-0.999) | <0.01 | 0.997(0.995-0.999) | <0.01 | |
| Alb(g/L) | 1.06(1.03-1.09) | <0.01 | 1.05(1.01-1.09) | 0.01 | |
| UA(μmol/L) | 0.995(0.993-0.997) | <0.01 | 0.997(0.994-0.999) | 0.01 | |
| TG(mmol/L) | 0.68(0.53-0.86) | <0.01 | - | ||
| TC(mmol/L) | 0.82(0.73-0.91) | <0.01 | - | ||
| Hb(g/L) | 0.98(0.97-0.99) | <0.01 | 0.97(0.95-0.98) | <0.01 | |
| Urinary sodium/Potassium ratio | 1.02(0.93-1.12) | 0.65 | - | ||
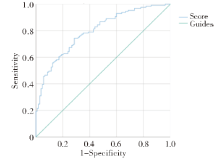
图2
4项指标联合模型鉴别ATIN与ATN的ROC曲线图
| [1] |
ULINSKI T, SELLIER-LECLERC A L, TUDORACHE E, et al. Acute tubulointerstitial nephritis[J]. Pediatr Nephrol, 2012, 27(7):1051-1057.
doi: 10.1007/s00467-011-1915-9 pmid: 21638156 |
| [2] |
JOYCE E, GLASNER P, RANGANATHAN S, et al. Tubulointerstitial nephritis: diagnosis, treatment, and monitoring[J]. Pediatr Nephrol, 2017, 32(4):577-587.
doi: 10.1007/s00467-016-3394-5 pmid: 27155873 |
| [3] | GEDIK G K, YILMAZ F, KAYA B, et al. Mercaptoacetyltriglycine renal scan for the differential diagnosis of acute tubular necrosis and interstitial nephritis associated to vancomycin[J]. Rev Esp Med Nucl Imagen Mol, 2012, 31(3):155-157. |
| [4] |
JOAQUIM A I, MENDES G E, RIBEIRO P F, et al. Ga-67 scintigraphy in the differential diagnosis between acute interstitial nephritis and acute tubular necrosis: an experimental study[J]. Nephrol Dial Transplant, 2010, 25(10):3277-3282.
doi: 10.1093/ndt/gfq152 URL |
| [5] | SCHWARTZ M M. Tubulointerstitial diseases and infections of the kidney[M]// JENNETTE J C, OLSON J L, SCHWARTZ M M, et al. 5th ed. Philadelphia: Lippincott Williams & Wilkins, 2015:657-890. |
| [6] |
PRAGA M, SEVILLANO A, AUÑÓN P, et al. Changes in the aetiology, clinical presentation and management of acute interstitial nephritis, an increasingly common cause of acute kidney injury[J]. Nephrol Dial Transplant, 2015, 30(9):1472-1479.
doi: 10.1093/ndt/gfu326 URL |
| [7] |
GOICOECHEA M, RIVERA F, LÓPEZ-GÓMEZ J M, et al. Increased prevalence of acute tubulointerstitial nephritis[J]. Nephrol Dial Transplant, 2013, 28(1):112-115.
doi: 10.1093/ndt/gfs143 URL |
| [8] |
BOMBACK A S, MARKOWITZ G S. Increased prevalence of acute interstitial nephritis: more disease or simply more detection?[J]. Nephrol Dial Transplant, 2013, 28(1):16-18.
doi: 10.1093/ndt/gfs318 URL |
| [9] |
KIM H, JO S K, AHN S Y, et al. Long-term renal outcome of biopsy-proven acute tubular necrosis and acute interstitial nephritis[J]. J Korean Med Sci, 2020, 35(26):e206.
doi: 10.3346/jkms.2020.35.e206 URL |
| [10] |
RUEBNER R L, FADROWSKI J J. Tubulointerstitial nephritis[J]. Pediatr Clin North Am, 2019, 66(1):111-119.
doi: 10.1016/j.pcl.2018.08.009 URL |
| [11] |
CHAWLA L S, BELLOMO R, BIHORAC A, et al. Acute kidney disease and renal recovery: consensus report of the Acute Disease Quality Initiative (ADQI) 16 Workgroup[J]. Nat Rev Nephrol, 2017, 13(4):241-257.
doi: 10.1038/nrneph.2017.2 pmid: 28239173 |
| [12] |
SU T, GU Y, SUN P, et al. Etiology and renal outcomes of acute tubulointerstitial nephritis: a single-center prospective cohort study in China[J]. Nephrol Dial Transplant, 2018, 33(7):1180-1188.
doi: 10.1093/ndt/gfx247 URL |
| [13] |
BAKER R J, PUSEY C D. The changing profile of acute tubulointerstitial nephritis[J]. Nephrol Dial Transplant, 2004, 19(1):8-11.
doi: 10.1093/ndt/gfg464 URL |
| [14] |
BUYSEN J G, HOUTHOFF H J, KREDIET R T, et al. Acute interstitial nephritis: a clinical and morphological study in 27 patients[J]. Nephrol Dial Transplant, 1990, 5(2):94-99.
doi: 10.1093/ndt/5.2.94 URL |
| [15] |
SCHWARZ A, KRAUSE P H, KUNZENDORF U, et al. The outcome of acute interstitial nephritis: risk factors for the transition from acute to chronic interstitial nephritis[J]. Clin Nephrol, 2000, 54(3):179-190.
pmid: 11020015 |
| [16] | 马杰, 文煜冰, 吴海婷, 等. 55例急性间质性肾炎的临床特点及病因分析[J]. 临床药物治疗杂志, 2021, 19(5):51-55. |
| MA J, WEN Y B, WU H T, et al. Clinical characteristics and etiological study of 55 patients with acute interstitial nephritis[J]. Clin Med J, 2021, 19(5):51-55. | |
| [17] | 刘小庆, 王墨. 199例儿童急性间质性肾炎临床及预后分析[J]. 重庆医科大学学报, 2020, 45(11):1573-1578. |
| LIU X Q, WANG M. Clinical and prognostic analysis of 199 children with acute interstitial nephritis[J]. J Chong-qing Med Univ, 2020, 45(11):1573-1578. | |
| [18] |
HOWELL M, SEBIRE N J, MARKS S D, et al. Biopsy-proven paediatric tubulointerstitial nephritis[J]. Pediatr Nephrol, 2016, 31(10):1625-1630.
doi: 10.1007/s00467-016-3374-9 pmid: 27139900 |
| [19] | 任海滨, 俞香宝, 孙彬, 等. 53例急性间质性肾炎临床病理分析[J]. 临床肾脏病杂志, 2013, 13(11):519-522. |
| REN H B, YU X B, SUN B, et al. Clinicopathological analysis of 53 cases of acute interstitial nephritis[J]. J Clin Nephrol, 2013, 13(11):519-522. | |
| [20] | 张燕京, 李晓玫. 药物相关肾实质性急性肾衰竭患者的贫血特征、红细胞生成素水平及其与肾损害的关系[J]. 北京大学学报(医学版), 2005, 37(5):471-475. |
| ZHANG Y J, LI X M. Relationship among the characteristics of anemia, serum level of erythropoietin and the renal tubulointerstitial injury in drug-associated renal parenchymal acute renal failure patients[J]. J Peking Univ (Health Sci) 2005, 37(5):471-475. | |
| [21] |
LEE T, YANG W S. Non-diabetic glycosuria as a diagnostic clue for acute tubulointerstitial nephritis in patients with azotemia[J]. Ren Fail, 2020, 42(1):1015-1021.
doi: 10.1080/0886022X.2020.1824923 pmid: 32985319 |
| [22] |
SALVADOR L G, CAROLINA G F, JESÚS R D, et al. A low BUN/creatinine ratio predicts histologically confirmed acute interstitial nephritis[J]. BMC Nephrol, 2023, 24(1):75.
doi: 10.1186/s12882-023-03118-0 pmid: 36967386 |
| [23] |
PERAZELLA M A, MARKOWITZ G S. Drug-induced acute interstitial nephritis[J]. Nat Rev Nephrol, 2010, 6(8):461-470.
doi: 10.1038/nrneph.2010.71 pmid: 20517290 |
| [24] |
URBSCHAT A, OBERMÜLLER N, HAFERKAMP A. Biomarkers of kidney injury[J]. Biomarkers, 2011, 16(Suppl 1):S22-S30.
doi: 10.3109/1354750X.2011.587129 URL |
| [25] |
MOLEDINA D G, WILSON F P, POBER J S, et al. Urine TNF-α and IL-9 for clinical diagnosis of acute interstitial nephritis[J]. JCI Insight, 2019, 4(10):e127456.
doi: 10.1172/jci.insight.127456 URL |
| [1] | 谢雅琼, 林孝怡. 血清游离轻链在鉴别诊断不同病因肾病的应用价值及其与患者肾功能分期的相关性分析[J]. 诊断学理论与实践, 2023, 22(02): 166-171. |
| [2] | 林霞, 高超, 黄沛, 王刚, 林国珍, 任汝静. 8例髓鞘少突胶质细胞糖蛋白抗体相关疾病患者的临床和影像学表现分析并文献复习[J]. 诊断学理论与实践, 2022, 21(05): 606-612. |
| [3] | 王昭晖, 吴海波. 胃神经鞘瘤31例临床病理学分析[J]. 诊断学理论与实践, 2021, 20(06): 552-556. |
| [4] | 史冬梅, 王晓琳, 陈璐, 谢青. 曼氏裂头蚴病52例临床特点及误诊分析[J]. 诊断学理论与实践, 2020, 19(1): 37-43. |
| [5] | 胡颖, 包玉洁, 白玉盘, 陆观珠, 成亚娇, 郭竹英, 许洁. 67例成人EB病毒感染临床及实验室特征分析[J]. 诊断学理论与实践, 2020, 19(1): 74-79. |
| [6] | 杨巧, 温玉婷, 杨昌伟. 伴浆膜腔积液的恶性黑色素瘤5例临床和细胞病理学检查分析[J]. 诊断学理论与实践, 2020, 19(05): 499-503. |
| [7] | 杜月月, 杜军, 沈倩, 葛绾宇, 吴海波. Warthin瘤样甲状腺乳头状癌1例及临床病理观察[J]. 诊断学理论与实践, 2020, 19(02): 188-190. |
| [8] | 王娟, 王楷文, 赵江峰. 抗MDA5抗体对皮肌炎继发间质性肺病的病情活动与预后评估的价值[J]. 诊断学理论与实践, 2019, 18(2): 155-159. |
| [9] | 王建军, 陈雅, 樊祥山, 牛丰南. 脾脏硬化性血管瘤样结节性转化8例临床病理分析及文献复习[J]. 诊断学理论与实践, 2019, 18(05): 560-564. |
| [10] | 忻笑容, 吴云林, 陈平, 谢玲, 周郁芬, 俞骁珺, 罗方秀, 项明. 胃癌608例临床及病理特征分析[J]. 诊断学理论与实践, 2019, 18(04): 470-472. |
| [11] | 常蕊, 徐嘉旭, 董海鹏, 吴梦雄, 赵雪松, 缪飞, 严福华. CT能谱成像在小肠克恩罗恩病活动度评估中的价值[J]. 诊断学理论与实践, 2019, 18(04): 432-435. |
| [12] | 杨茹雪, 李楠, 周婷, 赵艳, 陈少华, 朱清, 冯振中. 皮肤黑素细胞病变的临床病理分析[J]. 诊断学理论与实践, 2018, 17(05): 566-571. |
| [13] | 张祎昀, 徐雷, 唐兆生, 陈英华, 窦琴, 冯波. 2型糖尿病合并戊型肝炎患者的临床特征分析[J]. 诊断学理论与实践, 2018, 17(05): 557-561. |
| [14] | 杜海磊, 车嘉铭, 朱良纲, 李鹤成, 杭钧彪. 病理T1期浸润性肺腺癌不同病理亚型的临床特征及其预后分析[J]. 诊断学理论与实践, 2018, 17(01): 82-86. |
| [15] | 朱培培, 邹珏, 陈军, 徐蓉蓉, 颜红柱. 颅内孤立性纤维性肿瘤/血管周细胞瘤20例临床病理特征分析[J]. 诊断学理论与实践, 2017, 16(06): 622-626. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||