诊断学理论与实践 ›› 2023, Vol. 22 ›› Issue (04): 362-368.doi: 10.16150/j.1671-2870.2023.04.005
刘英婷, 易红梅( ), 王雪, 杨春雪, 欧阳斌燊, 许海敏, 王朝夫()
), 王雪, 杨春雪, 欧阳斌燊, 许海敏, 王朝夫()
收稿日期:2022-05-11
出版日期:2023-08-25
发布日期:2023-12-18
通讯作者:
王朝夫 E-mail: 基金资助:
LIU Yingting, YI Hongmei(), WANG Xue, YANG Chunxue, OUYANG Binshen XU Haimin, WANG Chaofu
Received:2022-05-11
Online:2023-08-25
Published:2023-12-18
摘要:
目的: 探讨十二指肠型滤泡性淋巴瘤(duodenal-type follicular lymphoma, DFL)的临床病理学特征及预后。方法: 回顾性分析17例DFL患者的临床特点、内镜表现、病理学特征及治疗方案,并进行随访。结果: 17例DFL患者中,男性8例,女性9例,男女比为1∶1.125,中位年龄为58岁(33~67岁),其中13例DFL患者是在常规体检中发现,内镜下多表现为颗粒状增生。DFL发生在十二指肠者有15例(88.2%),且全部位于十二指肠降段;单发病灶15例,多发病灶2例。内镜下,见病变位于黏膜层或黏膜下层,呈清楚或隐约的“膨胀性”生长,可见滤泡样结节,结节内由中心细胞样细胞和散在中心母细胞样细胞组成,相当于经典型滤泡性淋巴瘤的1级或2级。肿瘤细胞表达CD20、CD79a、CD10、BCL6及BCL2,9例患者的CD21染色显示滤泡树突网在肿瘤性滤泡周边密集、浓染,而在中央淡染、稀疏,Ki-67低表达。4例患者行第二代基因测序检测,其中3例共同检测到CREBBP基因变异。14例患者未经任何治疗,疾病无进展;1例行局部肠段切除,术后未行化疗和放疗,未复发;1例接受化疗加利妥昔单抗治疗,病变完全消退。结论: DFL多为单发病灶,镜下表现类似经典型滤泡性淋巴瘤1级或2级,较特殊的免疫表型是CD21常在肿瘤性滤泡周边更密集、深染,具有惰性生物学行为。
中图分类号:
刘英婷, 易红梅, 王雪, 杨春雪, 欧阳斌燊, 许海敏, 王朝夫. 十二指肠型滤泡性淋巴瘤17例临床病理特征及预后分析[J]. 诊断学理论与实践, 2023, 22(04): 362-368.
LIU Yingting, YI Hongmei, WANG Xue, YANG Chunxue, OUYANG Binshen XU Haimin, WANG Chaofu. Clinicopathological features and prognosis of 17 cases of duodenal-type follicular lymphoma[J]. Journal of Diagnostics Concepts & Practice, 2023, 22(04): 362-368.

图1
十二指肠型滤泡性淋巴瘤内镜下表现 a:十二指肠降段黏膜粗糙;b:空肠多发白色黏膜下隆起,与图a为同一例,表示为多发性病变;c:十二指肠降段凹陷处见可见白色颗粒样隆起呈簇分布;d:十二指肠降部乳头区域可见一不规则增殖性病灶,表面发红,凹凸不平,颗粒样改变。
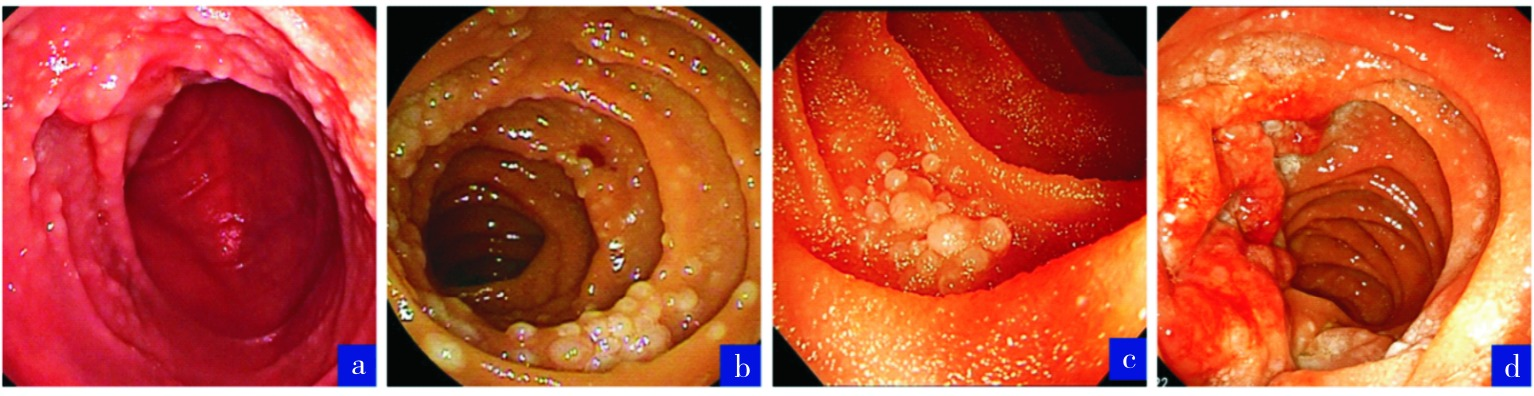
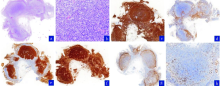
图2
十二指肠型滤泡性淋巴瘤的组织学病理HE形态及免疫表型特点 a:十二指肠黏膜层及黏膜下层内见多个滤泡样结节(HE,100×);b:滤泡样结节内可见两类细胞,主要是中心细胞样细胞,散在中心母细胞样细胞 (HE,400×);c:瘤细胞弥漫表达CD20;d.瘤细胞不表达CD3;e:瘤细胞CD10阳性,滤泡样结节外可见CD10阳性淋巴细胞;f:瘤细胞弥漫表达BCL2;g:CD21染色阳性,表现为滤泡周围强阳性;h:瘤细胞Ki-67增殖指数约10%。
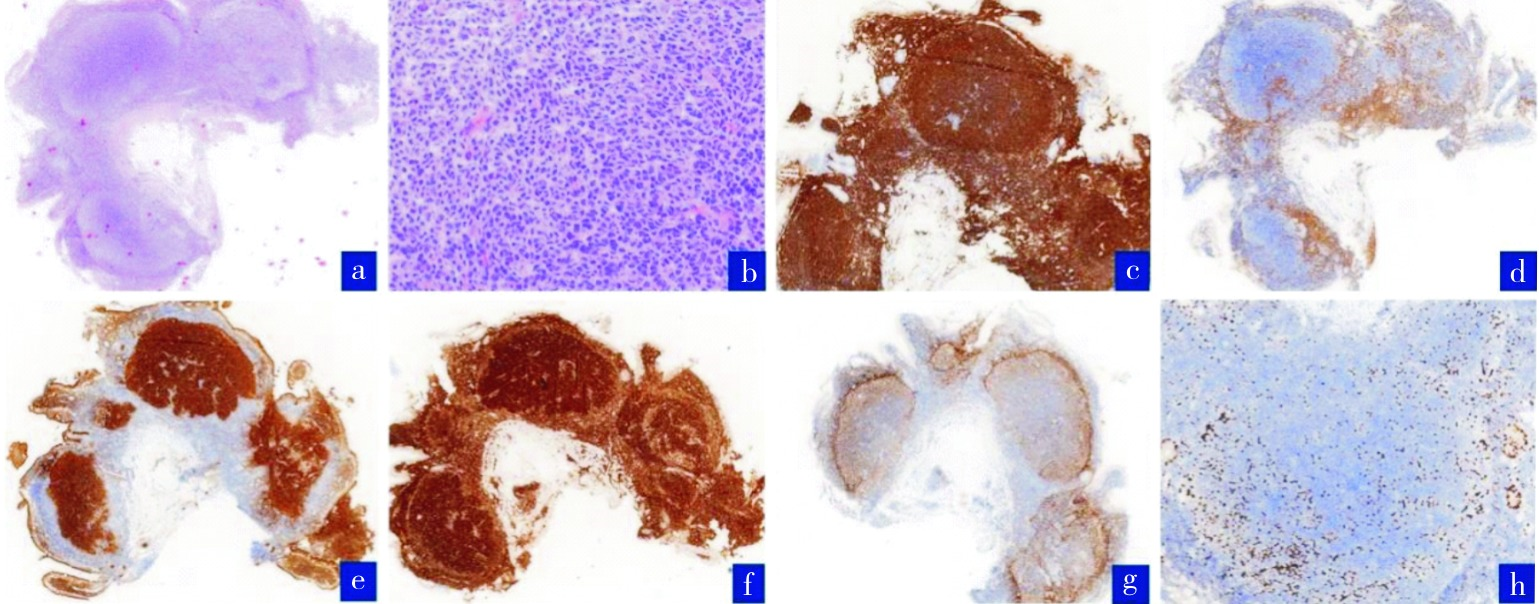

图3
十二指肠型滤泡性淋巴瘤的组织学病理HE形态及免疫表型特点 a:十二指肠黏膜层见一膨胀性生长的滤泡样结节(HE,100×);b:滤泡样结节内可见两类细胞,中心细胞样细胞和散在中心母细胞样细胞(HE,400×);c:瘤细胞弥漫表达CD20;d:瘤细胞表达CD10;e:滤泡样结节外可见CD10阳性淋巴细胞;f:瘤细胞表达BCL2;g:CD21染色阳性,表现为经典性滤泡性淋巴瘤的着色模式;h:瘤细胞Ki-67增殖指数约25%。

| [1] | SWERDLOW S H, World Health Organization, International Agency for Research on Cancer. WHO classification of tumours of haematopoietic and lymphoid tissues[M]. 4th. Lyon: International Agency for Research on Cancer, 2017. |
| [2] |
ANDERSON J R, ARMITAGE J O, WEISENBURGER D D. Epidemiology of the non-Hodgkin's lymphomas: distributions of the major subtypes differ by geographic locations. Non-Hodgkin's Lymphoma Classification Project[J]. Ann Oncol, 1998, 9(7):717-720.
doi: 10.1023/a:1008265532487 pmid: 9739436 |
| [3] |
SAITO M, MORI A, TSUKAMOTO S, et al. Duodenal-type follicular lymphoma more than 10 years after treatment intervention: A retrospective single-center analysis[J]. World J Gastrointest Oncol, 2022, 14(8):1552-1561.
doi: 10.4251/wjgo.v14.i8.1552 URL |
| [4] |
TAKATA K, TANINO M, ENNISHI D, et al. Duodenal follicular lymphoma: comprehensive gene expression analysis with insights into pathogenesis[J]. Cancer Sci, 2014, 105(5):608-615.
doi: 10.1111/cas.2014.105.issue-5 URL |
| [5] | SCHMATZ A I, STREUBEL B, KRETSCHMER-CHOTT E, et al. Primary follicular lymphoma of the duodenum is a distinct mucosal/submucosal variant of follicular lymphoma: a retrospective study of 63 cases[J]. J Clin Oncol, 2011, 29(11):1445-1451. |
| [6] |
TAKATA K, OKADA H, OHMIYA N, et al. Primary gastrointestinal follicular lymphoma involving the duodenal second portion is a distinct entity: a multicenter, retrospective analysis in Japan[J]. Cancer Sci, 2011, 102(8):1532-1536.
doi: 10.1111/cas.2011.102.issue-8 URL |
| [7] |
MORI M, KOBAYASHI Y, MAESHIMA A M, et al. The indolent course and high incidence of t(14;18) in primary duodenal follicular lymphoma[J]. Ann Oncol, 2010, 21(7):1500-1505.
doi: S0923-7534(19)39475-X pmid: 20022910 |
| [8] |
YOSHINO T, MIYAKE K, ICHIMURA K, et al. Increased incidence of follicular lymphoma in the duodenum[J]. Am J Surg Pathol, 2000, 24(5):688-693.
doi: 10.1097/00000478-200005000-00007 pmid: 10800987 |
| [9] |
SHIA J, TERUYA-FELDSTEIN J, PAN D, et al. Primary follicular lymphoma of the gastrointestinal tract: a clinical and pathologic study of 26 cases[J]. Am J Surg Pathol, 2002, 26(2):216-224.
pmid: 11812943 |
| [10] |
NAKAMURA S, MATSUMOTO T, UMENO J, et al. Endoscopic features of intestinal follicular lymphoma: the value of double-balloon enteroscopy[J]. Endoscopy, 2007, 39 Suppl 1:E26-E27.
doi: 10.1055/s-2007-966223 pmid: 17285496 |
| [11] |
HIGUCHI N, SUMIDA Y, NAKAMURA K, et al. Impact of double-balloon endoscopy on the diagnosis of jejunoi-leal involvement in primary intestinal follicular lymphomas: a case series[J]. Endoscopy, 2009, 41(2):175-178.
doi: 10.1055/s-0028-1119467 URL |
| [12] |
TAKATA K, SATO Y, NAKAMURA N, et al. Duodenal follicular lymphoma lacks AID but expresses BACH2 and has memory B-cell characteristics[J]. Mod Pathol, 2013, 26(1):22-31.
doi: 10.1038/modpathol.2012.127 URL |
| [13] |
TARI A, KITADAI Y, MOURI R, et al. Watch-and-wait policy versus rituximab-combined chemotherapy in Japanese patients with intestinal follicular lymphoma[J]. J Gastroenterol Hepatol, 2018, 33(8):1461-1468.
doi: 10.1111/jgh.2018.33.issue-8 URL |
| [14] |
MURAMATSU M, KINOSHITA K, FAGARASAN S, et al. Class switch recombination and hypermutation require activation-induced cytidine deaminase (AID), a potential RNA editing enzyme[J]. Cell, 2000, 102(5):553- 563.
pmid: 11007474 |
| [15] | LEUENBERGER M, FRIGERIO S, WILD P J, et al. AID protein expression in chronic lymphocytic leukemia/small lymphocytic lymphoma is associated with poor prognosis and complex genetic alterations[J]. Mod Pathol, 2010, 23(2):177-186. |
| [16] |
MUTO A, TASHIRO S, NAKAJIMA O, et al. The transcriptional programme of antibody class switching involves the repressor Bach2[J]. Nature, 2004, 429(6991):566-571.
doi: 10.1038/nature02596 |
| [17] |
SAKANE-ISHIKAWA E, NAKATSUKA S, TOMITA Y, et al. Prognostic significance of BACH2 expression in diffuse large B-cell lymphoma: a study of the Osaka Lymphoma Study Group[J]. J Clin Oncol, 2005, 23(31):8012-8017.
doi: 10.1200/JCO.2005.02.1626 URL |
| [18] |
TAKATA K, SATO Y, NAKAMURA N, et al. Duodenal and nodal follicular lymphomas are distinct: the former lacks activation-induced cytidine deaminase and follicular dendritic cells despite ongoing somatic hypermutations[J]. Mod Pathol, 2009, 22(7):940-949.
doi: 10.1038/modpathol.2009.51 URL |
| [19] |
MAMESSIER E, SONG J Y, EBERLE F C, et al. Early lesions of follicular lymphoma: a genetic perspective[J]. Haematologica, 2014, 99(3):481-488.
doi: 10.3324/haematol.2013.094474 pmid: 24162788 |
| [20] |
HELLMUTH J C, LOUISSAINT A JR, SZCZEPANOWSKI M, et al. Duodenal-type and nodal follicular lymphomas differ by their immune microenvironment rather than their mutation profiles[J]. Blood, 2018, 132(16):1695-1702.
doi: 10.1182/blood-2018-03-837252 pmid: 30126979 |
| [21] |
KAMIJO K, SHIMOMURA Y, YOSHIOKA S, et al. Clinical features and outcomes of duodenal-type follicular lymphoma: A single-center retrospective study[J]. EJHaem, 2022, 3(2):379-384.
doi: 10.1002/jha2.384 pmid: 35846028 |
| [22] | 陈青, 张燕林, 何妙侠, 等. 十二指肠型滤泡性淋巴瘤22例回顾性分析[J]. 临床与实验病理学杂志, 2019, 35(9):1112-1114. |
| CHEN Q, ZHANG Y L, HE M X, et al. Duodenal-type Follicular Lymphoma: A Retrospective Study of 22 Cases[J]. J Clin Exp Pathol, 2019, 35(9): 1112-1114. | |
| [23] |
TANIGAWA T, ABE R, KATO J, et al. Histological transformation in duodenal-type follicular lymphoma: a case report and review of the literature[J]. Oncotarget, 2019, 10(36):3424-3429.
pmid: 31164963 |
| [24] |
SENTANI K, MAESHIMA A M, NOMOTO J, et al. Follicular lymphoma of the duodenum: a clinicopathologic analysis of 26 cases[J]. Jpn J Clin Oncol, 2008, 38(8):547-552.
doi: 10.1093/jjco/hyn069 pmid: 18687756 |
| [25] |
KITABATAKE H, NAGAYA T, TANAKA N, et al. Development of diffuse large B-cell lymphoma from follicular lymphoma of the duodenum: changes in endoscopic findings during a 6-year follow-up[J]. Clin J Gastroenterol, 2017, 10(1):79-85.
doi: 10.1007/s12328-016-0697-9 pmid: 27873064 |
| [26] |
AKIYAMA S, IZUTSU K, OTA Y, et al. A case report of the histologic transformation of primary follicular lymphoma of the duodenum[J]. Medicine (Baltimore), 2014, 93(26):e165.
doi: 10.1097/MD.0000000000000165 URL |
| [27] |
HANGAI S, NAKAMURA F, KAMIKUBO Y, et al. Primary gastrointestinal follicular lymphoma with histological transformation[J]. Ann Hematol, 2013, 92(7):993-994.
doi: 10.1007/s00277-012-1654-4 pmid: 23271213 |
| [28] |
MIYATA-TAKATA T, TAKATA K, SATO Y, et al. A case of diffuse large B-cell lymphoma transformed from primary duodenal follicular lymphoma[J]. Pathol Int, 2014, 64(10):527-532.
doi: 10.1111/pin.2014.64.issue-10 URL |
| [29] |
SABURI M, KONDO Y, OGATA M, et al. Development of diffuse large B-cell lymphoma from duodenal type follicular lymphoma: a retrospective study of 23 cases[J]. Int J Hematol, 2020, 112(5):658-665.
doi: 10.1007/s12185-020-02957-z |
| [30] |
TARI A, ASAOKU H, TAKATA K, et al. The role of “watch and wait” in intestinal follicular lymphoma in rituximab era[J]. Scand J Gastroenterol, 2016, 51(3):321- 328.
doi: 10.3109/00365521.2015.1087589 URL |
| [1] | 李一林, 陈杨, 李艳艳, 冯旭娇, 章程, 李健, 沈琳. 循环肿瘤细胞检测在常见恶性肿瘤精准医学中的应用和展望[J]. 诊断学理论与实践, 2023, 22(04): 332-340. |
| [2] | 施仲伟. 从学术角度看高血压诊断界值不应下调至130/80 mmHg[J]. 诊断学理论与实践, 2023, 22(04): 348-361. |
| [3] | 张兰兰, 杨巧, 聂尊珍, 郭英. 胸膜SMARCA4缺失未分化肿瘤1例报告[J]. 诊断学理论与实践, 2023, 22(04): 389-392. |
| [4] | 刘益飞. DNA甲基化检测助力肿瘤早期筛查和诊断[J]. 诊断学理论与实践, 2023, 22(04): 393-401. |
| [5] | 胡静静, 沈银忠, 刘莉, 卢洪洲. 艾滋病合并播散性非结核分枝杆菌病诊治现状及研究进展[J]. 诊断学理论与实践, 2023, 22(04): 402-406. |
| [6] | 魏坚, 孙杰, 崔诗爽. 帕金森病早期诊断诺谟图模型的建立及验证[J]. 诊断学理论与实践, 2023, 22(03): 277-282. |
| [7] | 尹永芳, 唐永华, 梁妍, 陈志仁, 费晓春. Erdheim-Chester病6例临床及影像学特征分析[J]. 诊断学理论与实践, 2023, 22(03): 283-291. |
| [8] | 周晓蝶, 陈巍魏, 余波, 王璇, 王建军, 石群立, 饶秋, 鲍炜. 尿路上皮癌的临床病理学特征[J]. 诊断学理论与实践, 2023, 22(03): 292-299. |
| [9] | 李笑石, 秦越. 影像学技术在痛风诊断及疾病监测中的应用研究进展[J]. 诊断学理论与实践, 2023, 22(03): 311-318. |
| [10] | 吴娜明, 李军, 陶娟. 恶性黑色素瘤的诊断热点[J]. 诊断学理论与实践, 2023, 22(03): 215-220. |
| [11] | 徐莉, 高华杰, 杨梦歌, 李悦, 季苏琼. 合并抗TRIM21/Ro52抗体阳性的抗SRP阳性坏死性肌病患者临床特点分析[J]. 诊断学理论与实践, 2023, 22(03): 247-254. |
| [12] | 杨巧, 付欣, 王哲, 刘坦坦. 甲状腺继发性肿瘤细胞病理学特征[J]. 诊断学理论与实践, 2023, 22(03): 270-276. |
| [13] | 宋陆茜, 常春康. 2023年美国国立综合癌症网络(NCCN)《骨髓增生异常综合征临床实践指南》(第1版)解读[J]. 诊断学理论与实践, 2023, 22(02): 116-120. |
| [14] | 郝家琪, 王鑫鹭, 胡晓帆, 潘晓霞, 徐静, 马骏. 急性肾小管间质性肾炎与急性肾小管坏死的临床鉴别分析[J]. 诊断学理论与实践, 2023, 22(02): 127-133. |
| [15] | 颜凌, 王凌云, 陈勇, 杜联军. 双能CT图像深度学习重建算法在胃癌术前T分期中的应用[J]. 诊断学理论与实践, 2023, 22(02): 154-159. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||