诊断学理论与实践 ›› 2023, Vol. 22 ›› Issue (03): 270-276.doi: 10.16150/j.1671-2870.2023.03.10
杨巧1, 付欣2, 王哲2, 刘坦坦2,3( )
)
收稿日期:2022-11-24
出版日期:2023-06-25
发布日期:2023-11-17
通讯作者:
刘坦坦 E-mail:
YANG Qiao1, FU Xin2, WANG Zhe2, LIU Tantan2,3()
Received:2022-11-24
Online:2023-06-25
Published:2023-11-17
摘要:
目的:观察经超声引导下行细针抽吸术(fine-needle aspiration, FNA)细胞学检查诊断为甲状腺继发性肿瘤(secondary thyroid neoplasm, STN)及细胞学病理特征。方法:收集2011年1月至2021年5月期间空军军医大学第一附属医院病理科经FNA细胞学检查诊断为甲状腺恶性肿瘤的病例5 023例。对其中所有STN的FNA样本制作的传统涂片、液基制片和细胞蜡块,行苏木素-伊红(hematoxylin-eosin,HE)染色、巴氏染色和细胞免疫组织化学(immunohistochemistry,IHC)染色,并以甲状腺髓样癌涂片为对照,由2位高年资细胞病理专科医师,分析STN细胞病理学特征及细胞免疫组化特征,结合临床,总结STN与甲状腺髓样癌间的细胞病理鉴别要点。结果:5 023例甲状腺恶性肿瘤病例中,STN 8例(0.16%),甲状腺髓样癌33例(0.66%),甲状腺乳头状癌4 955例(98%),淋巴瘤16例(0.32%),鳞状细胞癌7例(0.14%),间变性癌及低分化癌各2例(0.04%)。33例髓样癌细胞形态多样,呈浆细胞样、上皮样、梭形,可见少量奇异性巨细胞,且背景中可见淀粉样物。8例STN均无典型甲状腺乳头状癌的细胞核特征;1例转移性肺腺癌可见三维立体乳头状结构及腺样结构;4例转移性鳞状细胞癌可见成簇或散在分布的异型鳞状细胞,结合其各自的特征性免疫表型,可明确诊断;2例转移性乳腺癌、1例转移性肺小细胞癌则与甲状腺髓样癌间的细胞学形态特征有部分重叠,细胞均体积小、深染,需要检测免疫组化标志物雌激素受体(estrogen receptor,ER)、孕激素受体(progesterone receptor PR)、细胞角蛋白7(cytokeratin7,CK7)、GATA3、突触素(synaptophysin,Syn)、神经细胞黏附分子(neural cell adhesion molecule,CD56)、嗜铬素A(chromogranin A,CgA)、降钙素(calcitonin,CT)、甲状腺球蛋白(thyroglobulin,TG)、甲状腺转录因子-1(thyroid transcription-1,TTF-1)、配对盒基因8(paired box gene 8,PAX-8)等,并综合临床病史进行鉴别。结论:本组样本中,STN仅占甲状腺恶性肿瘤的0.16%,较少见,对于有髓样癌表现的病例,要注意乳腺癌、肺癌性STN可能,需结合免疫组化及病史进行鉴别诊断。
中图分类号:
杨巧, 付欣, 王哲, 刘坦坦. 甲状腺继发性肿瘤细胞病理学特征[J]. 诊断学理论与实践, 2023, 22(03): 270-276.
YANG Qiao, FU Xin, WANG Zhe, LIU Tantan. Cytopathologic analysis of thyroid secondary tumors[J]. Journal of Diagnostics Concepts & Practice, 2023, 22(03): 270-276.
表1
甲状腺继发性肿瘤患者的临床资料
| Sex | Age (years) | History disease | Ultrasound results | Follow-up (months) | |
|---|---|---|---|---|---|
| 1 | Female | 57 | / | Right, mixed echo region, 1.9cm×1.5cm | 1 |
| 2 | Female | 64 | Small cell carcinoma of the left lung, 2 years and 8 months, cervical lymph node metastasis lasted 6 months | Right, low echo area, 2.4cm×1.4cm | 24 (death) |
| 3 | Female | 56 | Breast cancer, 5 years and 6 months | Isthmus to the right, Low echo area, 1.7cm×1.2cm | 29 |
| 4 | Female | 58 | Breast cancer, eight years and ten months | Right, low echo area, 2.2cm×1.5cm | 18 |
| 5 | Male | 56 | Squamous cell carcinoma of larynx, 1 year | Right, low echo area, 0.9cm×0.8cm | 24 |
| 6 | Male | 68 | Squamous cell carcinoma of the esophagus, 3 years | Right, low echo area, 1.5cm×1.2cm | 60 (death) |
| 7 | Male | 75 | Squamous cell carcinoma of hypopharynx, 4 years and 2 months | Right, low echo area, 3.2cm×3.7cm | 81 |
| 8 | Male | 64 | Squamous cell carcinoma of the trachea, 5 days | Right, low echo area, 2.8cm×2.6cm | 48 |
表2
STN与甲状腺髓样癌间的细胞形态学特征及免疫表型比较
| Number of cases | Normal follicles in the background | Arrangement mode | Cytological characteristics | Nuclear chromatin | Positive (IHC) | Negative (IHC) | |
|---|---|---|---|---|---|---|---|
| Adenocarci- noma of lung | 1 | Occasionally | Three-dimensional adenoid structure, papillary structure | Large, abundant cytoplasm, visible mucous vacuoles | Obvious nucleolus | CK7、TTF-1、NapsinA | CA125、WT-1、TG、PAX-8 |
| Small cell carci- noma of lung | 1 | Massive necrosis, apoptosis | Clustered,scattered, Mosaic-like | Uniform size, bare nucleus | Pepper salt like, fine granular | Syn、CD56、CgA | CT、TG |
| Breast cancer | 2 | Not seen | Clumps, clusters, scattered | Difference in size, The cytoplasm is medium to abundant with occasional vacuoles | Hyperchromatic nuclei, nucleolus were not obvious | ER、PR、CK7、GATA3 | TTF-1、PAX-8、CT |
| Squamous cell carcinoma | 4 | More or less, Neutrophils visible | Lamellar, nestlike, scattered | Significant size difference, round or fusiform, cytoplasmic keratosis is common | Hyperchromatic nuclei, polygon, irregular nuclear membranes | P63、P40 | TG |
| Medullary thyr- oid carcinoma | 33 | More or less | Single scattered, cell boundaries is unclear | Plasmacytoid, epithelioid, strange giant cell | Pepper salt like, fine granular | Syn、CD56、CgA、CT | TG |
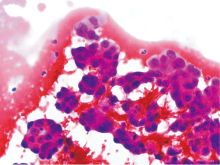
图1
病例1,甲状腺转移性肺腺癌(FNA) 注:肿瘤细胞形成三维立体腺样结构或乳头状结构,细胞核大、淡染,核仁明显,胞质丰富(HE,×400)。
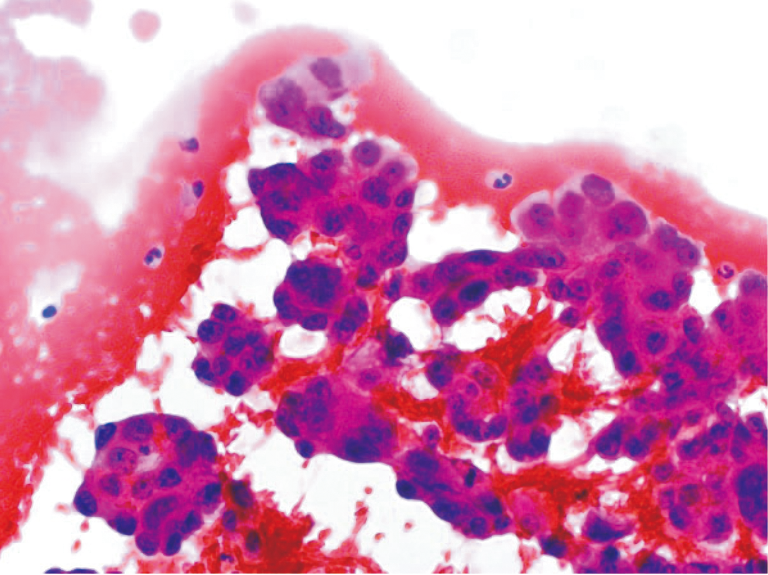
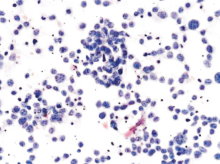
图2
病例2,甲状腺转移性肺小细胞癌(FNA) 注:肿瘤细胞大小较一致、裸核样,染色质细颗粒状、胡椒盐样,散在或呈簇状分布(HE,×400)。
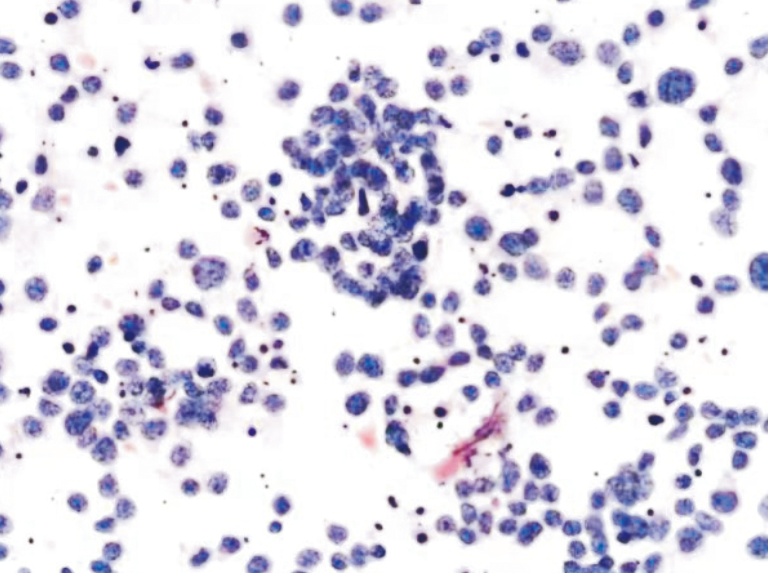
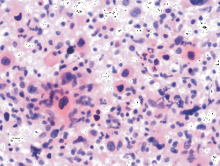
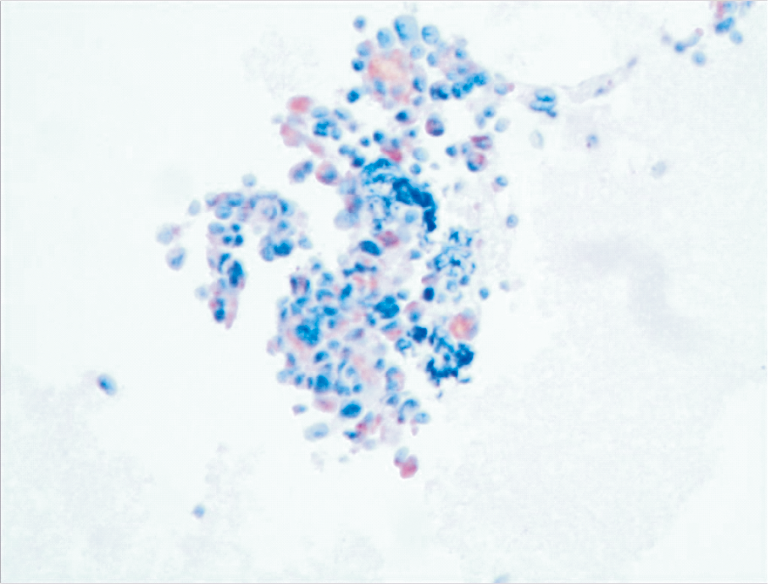
图3
病例8,甲状腺转移性鳞状细胞癌 注:肿瘤细胞单个散在分布,细胞核大小不一、浓染,胞浆丰富、嗜酸性,可见胞浆角化(HE,×400)。
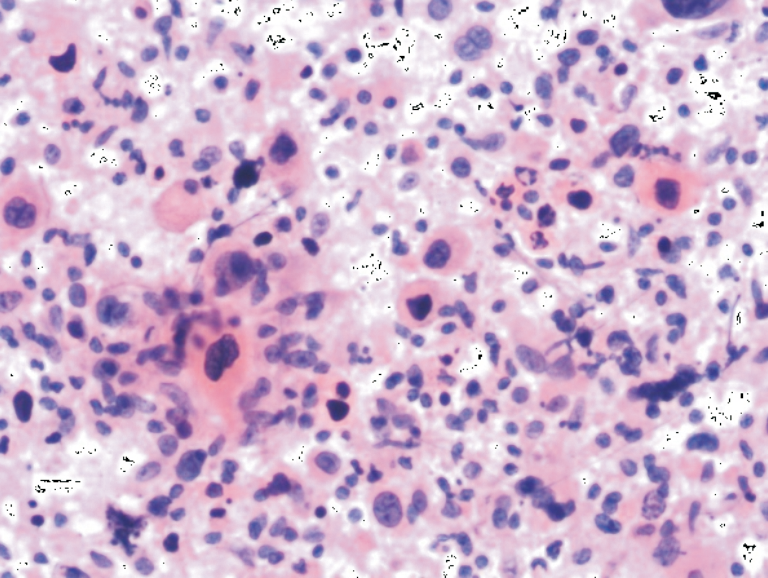
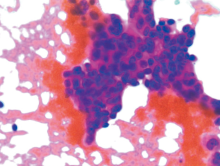
图4
病例4,甲状腺转移性乳腺癌 注:肿瘤细胞片状分布,细胞核大小不一,深染,形态不规则(HE,×400)。
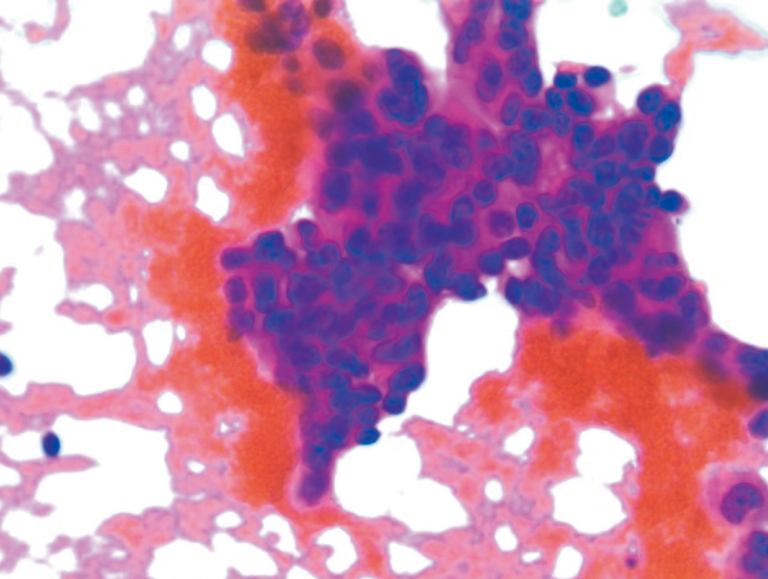
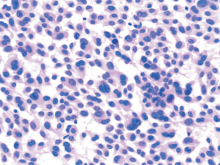
图5
髓样癌(HE,×400) 注:肿瘤细胞散在分布为主,呈上皮样、浆细胞样,可见奇异形巨细胞。
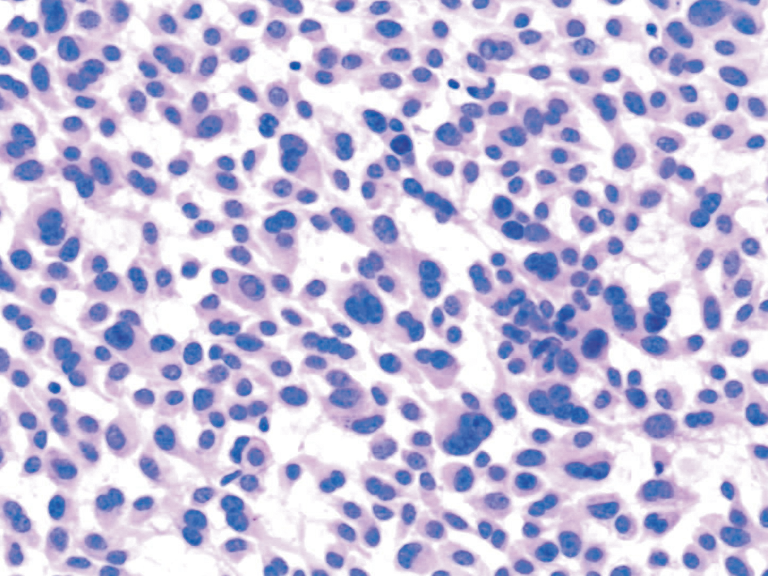
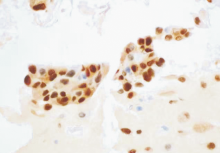
图6
乳腺癌细胞(病例4)(IHC,×400) 注:ER阳性
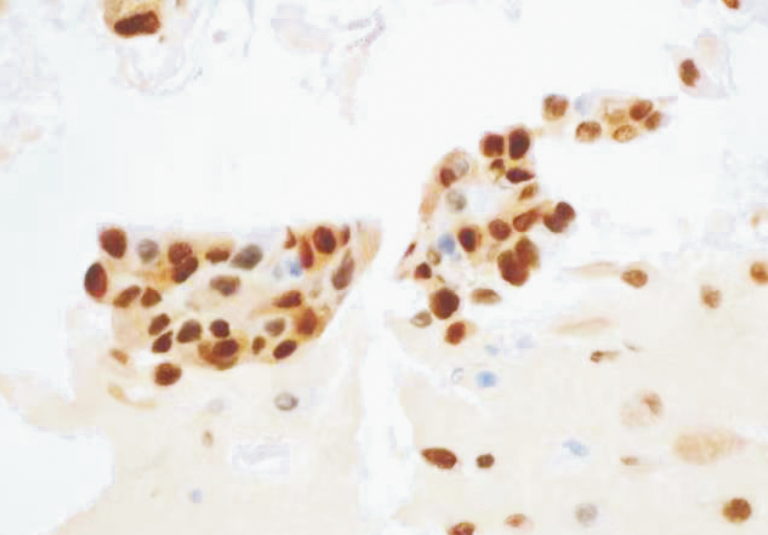
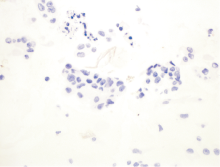
图7
乳腺癌细胞(病例4)(IHC,×400) 注:CT阴性
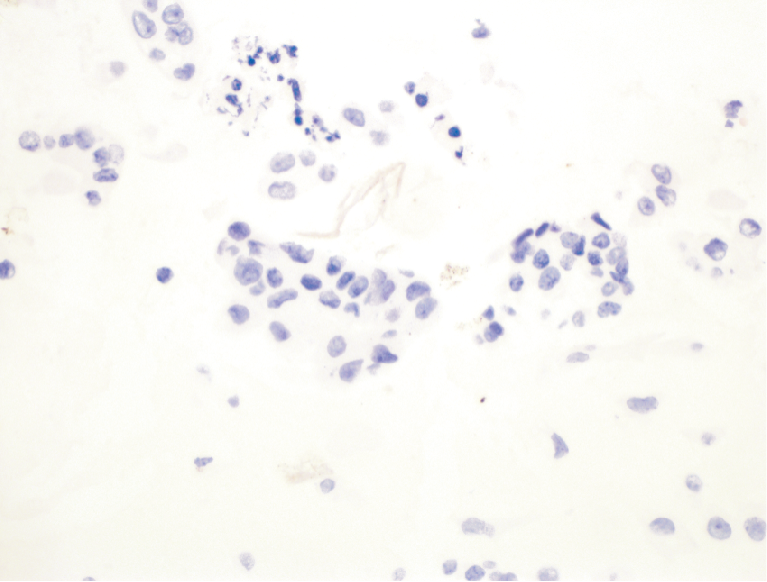
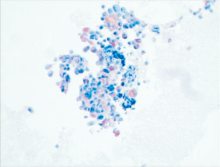
图8
髓样癌(IHC,×400) 注:CT阳性
| [1] |
PUSZTASZERI M, WANG H, CIBAS E S, et al. Fine-needle aspiration biopsy of secondary neoplasms of the thyroid gland: a multi-institutional study of 62 cases[J]. Cancer Cytopathol, 2015, 123(1):19-29.
doi: 10.1002/cncy.21494 pmid: 25369542 |
| [2] |
MIRALLIÉ E, RIGAUD J, MATHONNET M, et al. Mana-gement and prognosis of metastases to the thyroid gland[J]. J Am Coll Surg, 2005, 200(2):203-207.
doi: 10.1016/j.jamcollsurg.2004.10.009 URL |
| [3] |
ZHANG L, LIU Y, LI X, et al. Metastases to the thyroid gland: A report of 32 cases in PUMCH[J]. Medicine (Baltimore), 2017, 96(36):e7927.
doi: 10.1097/MD.0000000000007927 URL |
| [4] |
BATTISTELLA E, POMBA L, MATTARA G, et al. Metastases to the thyroid gland: review of incidence, clinical presentation, diagnostic problems and surgery, our experience[J]. J Endocrinol Invest, 2020, 43(11):1555-1560.
doi: 10.1007/s40618-020-01282-w |
| [5] |
HOOKIM K, GAITOR J, LIN O, et al. Secondary tumors involving the thyroid gland: A multi-institutional analysis of 28 cases diagnosed on fine-needle aspiration[J]. Diagn Cytopathol, 2015, 43(11):904-911.
doi: 10.1002/dc.23331 pmid: 26302896 |
| [6] |
HEGEROVA L, GRIEBELER M L, REYNOLDS J P, et al. Metastasis to the thyroid gland: report of a large series from the Mayo Clinic[J]. Am J Clin Oncol, 2015, 38(4):338-342.
doi: 10.1097/COC.0b013e31829d1d09 URL |
| [7] |
KIM T Y, KIM W B, GONG G, et al. Metastasis to the thyroid diagnosed by fine-needle aspiration biopsy[J]. Clin Endocrinol (Oxf), 2005, 62(2):236-241.
doi: 10.1111/cen.2005.62.issue-2 URL |
| [8] |
BUŁA G, WALER J, NIEMIEC A, et al. Diagnosis of metastatic tumours to the thyroid gland by fine needle aspiration biopsy[J]. Endokrynol Pol, 2010, 61(5):427-429.
pmid: 21049452 |
| [9] |
PAPI G, FADDA G, CORSELLO S M, et al. Metastases to the thyroid gland: prevalence, clinicopathological aspects and prognosis: a 10-year experience[J]. Clin Endocrinol (Oxf), 2007, 66(4):565-571.
doi: 10.1111/cen.2007.66.issue-4 URL |
| [10] |
NIXON I J, COCA-PELAZ A, KALEVA A I, et al. Metastasis to the Thyroid Gland: A Critical Review[J]. Ann Surg Oncol, 2017, 24(6):1533-1539.
doi: 10.1245/s10434-016-5683-4 pmid: 27873099 |
| [11] |
MONTERO P H, IBRAHIMPASIC T, NIXON I J, et al. Thyroid metastasectomy[J]. J Surg Oncol, 2014, 109(1):36-41.
doi: 10.1002/jso.23452 pmid: 24122778 |
| [12] |
KO H M, JHU I K, YANG S H, et al. Clinicopathologic analysis of fine needle aspiration cytology of the thyroid. A review of 1,613 cases and correlation with histopathologic diagnoses[J]. Acta Cytol, 2003, 47(5):727-732.
doi: 10.1159/000326596 URL |
| [13] |
CIRIANO HERNÁNDEZ P, MARTÍNEZ PINEDO C, CALCERRADA ALISES E, et al. Colorectal cancer metastases to the thyroid gland: A case report[J]. World J Gastrointest Surg, 2020, 12(3):116-122.
doi: 10.4240/wjgs.v12.i3.116 pmid: 32218894 |
| [14] |
MANATAKIS D K, TASIS N, ANTONOPOULOU M I, et al. Colorectal cancer metastases to the thyroid gland-a systematic review : Colorectal cancer thyroid metastases[J]. Hormones (Athens), 2021, 20(1):85-91.
doi: 10.1007/s42000-020-00255-1 pmid: 33150571 |
| [15] |
WOOD K, VINI L, HARMER C. Metastases to the thyroid gland: the Royal Marsden experience[J]. Eur J Surg Oncol, 2004, 30(6):583-588.
doi: 10.1016/j.ejso.2004.03.012 URL |
| [16] |
CHUNG A Y, TRAN T B, BRUMUND K T, et al. Metastases to the thyroid: a review of the literature from the last decade[J]. Thyroid, 2012, 22(3):258-268.
doi: 10.1089/thy.2010.0154 pmid: 22313412 |
| [17] |
GHOSSEIN C A, KHIMRAJ A, DOGAN S, et al. Metastasis to the thyroid gland: a single-institution 16-year experience[J]. Histopathology, 2021, 78(4):508-519.
doi: 10.1111/his.v78.4 URL |
| [18] |
ROMERO ARENAS M A, RYU H, LEE S, et al. The role of thyroidectomy in metastatic disease to the thyroid gland[J]. Ann Surg Oncol, 2014, 21(2):434-439.
doi: 10.1245/s10434-013-3282-1 pmid: 24081800 |
| [1] | 李笑石, 秦越. 影像学技术在痛风诊断及疾病监测中的应用研究进展[J]. 诊断学理论与实践, 2023, 22(03): 311-318. |
| [2] | 吴娜明, 李军, 陶娟. 恶性黑色素瘤的诊断热点[J]. 诊断学理论与实践, 2023, 22(03): 215-220. |
| [3] | 郝家琪, 王鑫鹭, 胡晓帆, 潘晓霞, 徐静, 马骏. 急性肾小管间质性肾炎与急性肾小管坏死的临床鉴别分析[J]. 诊断学理论与实践, 2023, 22(02): 127-133. |
| [4] | 谢雅琼, 林孝怡. 血清游离轻链在鉴别诊断不同病因肾病的应用价值及其与患者肾功能分期的相关性分析[J]. 诊断学理论与实践, 2023, 22(02): 166-171. |
| [5] | 王昭晖, 吴海波. 胃神经鞘瘤31例临床病理学分析[J]. 诊断学理论与实践, 2021, 20(06): 552-556. |
| [6] | 杨巧, 温玉婷, 杨昌伟. 伴浆膜腔积液的恶性黑色素瘤5例临床和细胞病理学检查分析[J]. 诊断学理论与实践, 2020, 19(05): 499-503. |
| [7] | 杜月月, 杜军, 沈倩, 葛绾宇, 吴海波. Warthin瘤样甲状腺乳头状癌1例及临床病理观察[J]. 诊断学理论与实践, 2020, 19(02): 188-190. |
| [8] | 王建军, 陈雅, 樊祥山, 牛丰南. 脾脏硬化性血管瘤样结节性转化8例临床病理分析及文献复习[J]. 诊断学理论与实践, 2019, 18(05): 560-564. |
| [9] | 常蕊, 徐嘉旭, 董海鹏, 吴梦雄, 赵雪松, 缪飞, 严福华. CT能谱成像在小肠克恩罗恩病活动度评估中的价值[J]. 诊断学理论与实践, 2019, 18(04): 432-435. |
| [10] | 杨茹雪, 李楠, 周婷, 赵艳, 陈少华, 朱清, 冯振中. 皮肤黑素细胞病变的临床病理分析[J]. 诊断学理论与实践, 2018, 17(05): 566-571. |
| [11] | 朱培培, 邹珏, 陈军, 徐蓉蓉, 颜红柱. 颅内孤立性纤维性肿瘤/血管周细胞瘤20例临床病理特征分析[J]. 诊断学理论与实践, 2017, 16(06): 622-626. |
| [12] | 符蓉, 王朝夫, 欧阳斌燊. 软骨母细胞瘤21例临床病理及影像学特征分析[J]. 诊断学理论与实践, 2017, 16(05): 537-539. |
| [13] | 衣琳, 肖立, 陈燕, 殷于磊. 间变性大细胞淋巴瘤临床病理特征分析[J]. 诊断学理论与实践, 2017, 16(03): 313-319. |
| [14] | 张晶, 周军, 孙林德, 赵志华,. 肾脏上皮样血管平滑肌脂肪瘤9例临床病理分析[J]. 诊断学理论与实践, 2016, 15(03): 297-301. |
| [15] | 杨林花,. 巨幼细胞贫血的诊断[J]. 诊断学理论与实践, 2015, 14(05): 483-486. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||