诊断学理论与实践 ›› 2024, Vol. 23 ›› Issue (06): 587-593.doi: 10.16150/j.1671-2870.2024.06.005
张俊花1,2, 李一林3, 谢静远2, 张春丽2, 徐静2( )
)
收稿日期:2024-06-27
出版日期:2024-12-25
发布日期:2024-12-25
通讯作者:
徐静 E-mail:xjjesse@126.com基金资助:
ZHANG Junhua1,2, LI Yilin3, XIE Jingyuan2, ZHANG Chunli2, XU Jing2()
Received:2024-06-27
Published:2024-12-25
Online:2024-12-25
摘要:
目的: 分析C3肾小球病(C3 glomerulopathy,C3G)的临床预后相关病理特征。方法: 收集2012年至2022年于上海交通大学医学院附属瑞金医院肾内科住院且经肾活检组织学诊断为C3G的所有病例,共7例,回顾性分析其临床、病理及随访资料,观察预后相关病理特征。结果: 7例C3G患者(男/女,3/4),中位起病年龄51岁,中位确诊年龄为54岁,中位随访时间为84个月(48~144个月),2例(例1、例7)失随访,2例(例5、例6)预后不良,3例(例2~4)预后良好。临床表现,2例(例3、例7)为肾病综合征,3例(例1、例3、例6)伴肾功能不全,6例(例1~6)伴有血尿,7例均表现为低补体血症伴高血压,均无明显肾外表现。长期随访患者5例,随访至2年时,1例(例3)尿蛋白及肌酐完全缓解,3例(例2、例4、例5)尿蛋白及肾功能稳定,1例(例6)尿蛋白增加、肾功能下降。随访至6年时,2例预后较好(例2、例4),1例(例3)因尿蛋白及肌酐完全缓解停止随访,1例(例6)在随访2年时预后差的基础上尿蛋白进一步增加,肾功能明显下降,1例(例5)新进展至大量尿蛋白。随访6年时,回顾肾脏病理,3例(例2~4)预后好的病例,光镜下以弥漫毛细血管内皮细胞增生伴毛细血管管腔内中性粒细胞浸润为主要表现,而肾小球球性硬化及肾小球基底膜假双轨表现不明显,且电镜下系膜区电子致密物沉积较少;2例(例5、例6)预后差的病例,以光镜下肾小球球性硬化比例升高[大于(年龄-20)/2×100%]、大量肾小球基底膜假双轨,电镜下系膜区大量电子致密物沉积为主要表现,而毛细血管内皮细胞增生伴毛细血管腔内中性粒细胞及嗜酸性粒细胞浸润较少。结论: C3G组织病理以急性病变(肾小球毛细血管内皮细胞增生、管腔中性粒细胞浸润等)为主要表现者,预后较好,可予以激素、免疫抑制剂为主的积极治疗;C3G组织病理表现以慢性病变( 肾小球球性硬化、肾小球基底膜假双轨形成、系膜区电子致密物大量沉积等)为主要表现,患者则预后不良,建议予以保守治疗,避免过度治疗。
中图分类号:
张俊花, 李一林, 谢静远, 张春丽, 徐静. C3肾病临床预后相关病理特征分析[J]. 诊断学理论与实践, 2024, 23(06): 587-593.
ZHANG Junhua, LI Yilin, XIE Jingyuan, ZHANG Chunli, XU Jing. Analysis of pathological features related to clinical prognosis in C3 glomerulopathy[J]. Journal of Diagnostics Concepts & Practice, 2024, 23(06): 587-593.
表1
患者临床资料
| Index | case1 | case2 | case3 | case4 | case5 | case6 | case7 |
|---|---|---|---|---|---|---|---|
| Baseline data | |||||||
| Gender | Female | Female | Female | Female | Male | Male | Male |
| Age of onset(years) | 51 | 42 | 58 | 18 | 54 | 58 | 26 |
| Age at diagnosis(years) | 51 | 54 | 64 | 23 | 57 | 58 | 29 |
| Follow up(months) | 3 | 108 | 48 | 72 | 144 | 84 | 0 |
| Family history | No | No | No | No | No | No | No |
| SP(mmHg) | 137 | 118 | 128 | 120 | 124 | 180 | 138 |
| DP(mmHg) | 81 | 90 | 89 | 74 | 86 | 96 | 85 |
| NS | No | No | Yes | No | No | No | Yes |
| 24 h TUP(mg) | 2274 | 1632 | 4092 | 1508 | 877 | 1538 | 6301 |
| Microscopic hematuria(/HP) | 11-15 | 6-11 | 4-5 | Full field | 6-10 | 4-5 | 0 |
| Scr(μmol/L) | 175 | 55 | 102 | 47 | 94 | 113 | 78 |
| eGFR(mL/min) | 28.6 | 114.5 | 49.2 | 134.1 | 79.8 | 61.4 | 116 |
| sAlb(g/L) | 25 | 26 | 26 | 30 | 30 | 33 | 29 |
| C3(g/L) | 0.28 | 0.06 | 0.6 | 0.6 | 0.56 | 0.62 | 0.43 |
| C4(g/L) | 0.1 | 0.1 | 0.18 | 0.12 | 0.12 | 0.2 | 0.18 |
| Hb(g/L) | 119 | 113 | 92 | 108 | 115 | 122 | 150 |
| Therapy | MMF+P | ARB+P | ARB+P+CYC | ARB | ARB+P+MMF | ARB | ARB+P+CYC |
| Remission time(months) | 3 | 3 | 2 | 3 | 32 | No | NA |
| Relapse(months) | NA | 18 | No | 46 | 67 | No | NA |
| Follow up for 2 years data | |||||||
| Therapy | NA | ARB+P+CNI | ARB | ARB | ARB+P+MMF | ARB+P+MMF | NA |
| 24 h TUP(mg) | NA | 1542 | 155 | 954 | 352 | 2273 | NA |
| Scr(μmol/L) | NA | 62 | 78 | 54 | 100 | 157 | NA |
| eGFR(ml/min) | NA | 991 | 68.1 | 142.1 | 72.6 | 43.25 | NA |
| sAlb(g/L) | NA | 29 | 42 | 33 | 35 | 27 | NA |
| C3(g/L) | NA | 0.06 | NA | 0.08 | 0.64 | NA | NA |
| C4(g/L) | NA | 0.1 | NA | 0.1 | 0.1 | NA | NA |
| Follow up for 6 years data | |||||||
| Therapy | NA | ARB+P+CNI | NA | ARB | ARB+P+RTX | ARB+P+MMF | NA |
| 24 h TUP(mg) | NA | 1236 | NA | 354 | 6013 | 3627 | NA |
| Scr(μmol/L) | NA | 69 | NA | 51 | 131 | 202 | NA |
| eGFR(mL/min) | NA | 96 | NA | 126.9 | 53.5 | 29.2 | NA |
| sAlb(g/L) | NA | 29 | NA | 39 | 17 | 26 | NA |
| C3(g/L) | NA | 0.07 | NA | 0.46 | 0.59 | NA | NA |
| C4(g/L) | NA | 0.1 | NA | 0.2 | 0.2 | NA | NA |
表2
患者活检组织学特征
| Index | case1 | case2* | case3* | case4* | case5 | case6 | case7 |
|---|---|---|---|---|---|---|---|
| Light microscope(LM) | |||||||
| Glomerulus(n) | 36 | 6 | 33 | 29 | 19 | 22 | 39 |
| Glomerulosclerosis(n,%) | 2(5.6) | 0(0) | 3(9) | 0(0) | 3(15.8) | 5(26.3)↑ | 12(30.8)↑ |
| Segmental sclerosis(n) | 2 | 0 | 0 | 2 | 0 | 0 | 5 |
| Endocapillary proliferation | ↑ | ↑ | ↑ | ↑ | no | no | no |
| Neutrophils in capillaries | ↑ | ↑ | ↑ | ↑ | no | no | no |
| GBM pseudo double track | non-Dif | non-Dif | non-Dif | non-Dif | Dif | Dif | Dif |
| Mesangial matrix increased | sev | sev | sev | sev | mod | sev | sev |
| Mesangial cells increased | mild | sev | sev | sev | mod | sev | mod |
| Interstitial fibrosis | mild | mild | mild | mild | mild | mod | mod |
| Tubules atrophic | mild | mild | mild | mild | mild | mod | mod |
| Interstitial inflammatory cell | mild | mild | sev | mild | mild | mod | mod |
| Immunofluorescence(IF) | |||||||
| Deposition of C3 | mod | sev | sev | sev | mod | mod | mod |
| Other immune complexes | no | ↑ | no | ↑ | no | ↑ | no |
| Electron microscope(EM) | |||||||
| Electron dense deposits | |||||||
| Mesangial zone | mild | mild | mild | no | sev | mod | mod |
| Epithelial side | no | mild | mild | no | no | no | mod |
| Subepithelial | no | no | mild | mild | mild | mod | mod |
| GBM | no | no | mild | no | no | no | mod |
| Foot process fusion | Dif | Dif | Dif | no | Dif | no | Dif |

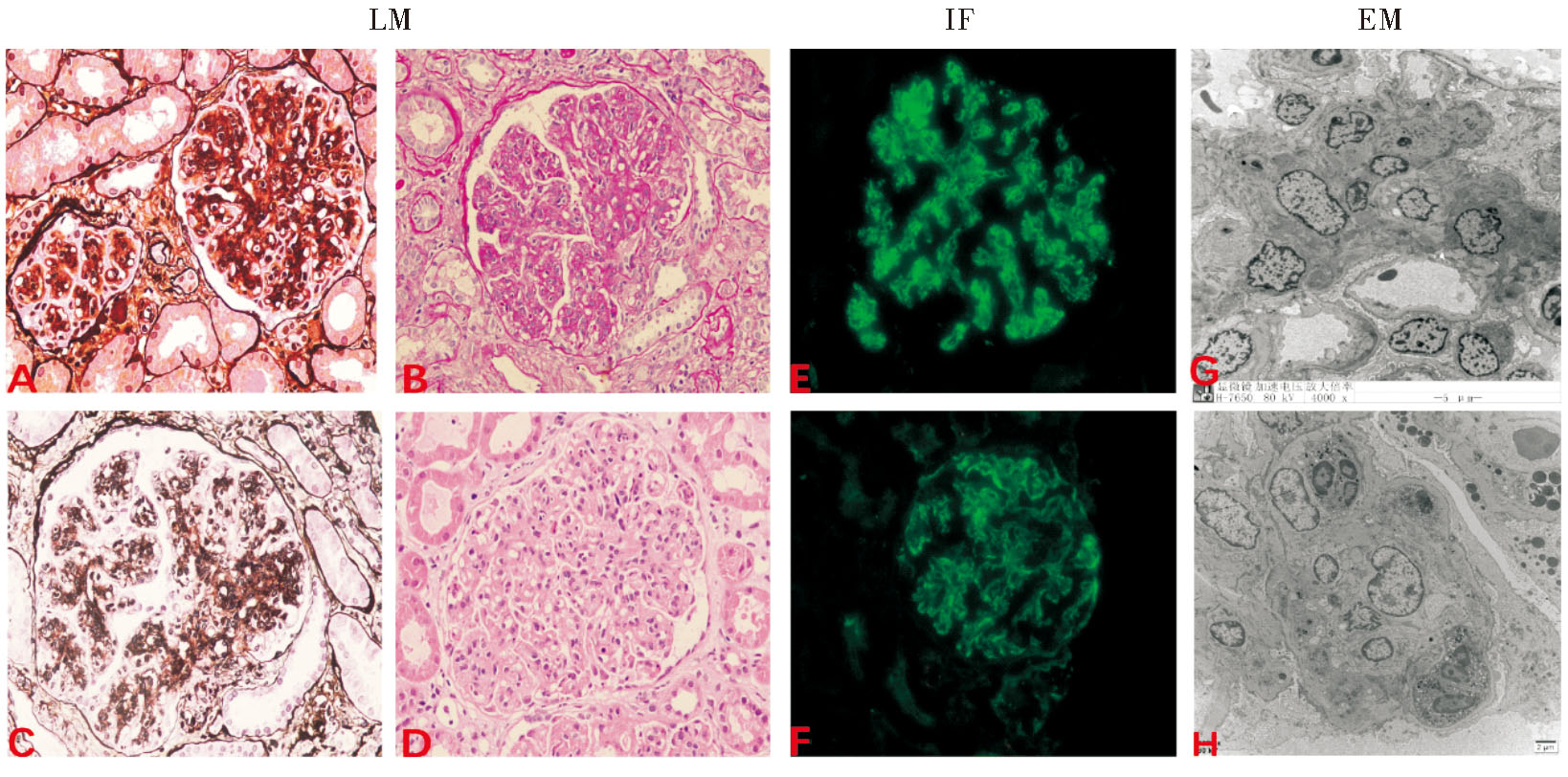
图1
C3G肾脏病理表现 注:A:银染色可见肾小球基底膜弥漫双轨(×400);B:过碘酸雪夫染色可见弥漫毛细血管内细胞增多(×400);C:银染色可见肾小球基底膜节段双轨(×400);D:苏木素-伊红染色可见肾小球毛细血管腔内中性粒细胞浸润(×400);E:冰冻免疫荧光C3(+++),毛细血管襻、系膜区,弥漫性(×400);F:冰冻免疫荧光C3(+~++),毛细血管襻、系膜区,弥漫性(×400);G:电镜下弥漫系膜细胞增生、弥漫系膜区电子致密物沉积(×2 000);H:电镜下弥漫毛细血管腔内炎细胞浸润(×4 000)
| [1] | MEHDI A, TALIERCIO J J. C3 glomerulopathy[J]. Cleve Clin J Med, 2023, 90(6 suppl 1):e1-e4. |
| [2] |
SETHI S, DE VRIESE A S, FERVENZA F C. Acute glomerulonephritis[J]. Lancet, 2022, 399(10335):1646-1663.
doi: 10.1016/S0140-6736(22)00461-5 pmid: 35461559 |
| [3] | DE VRIESE A S, SETHI S, VAN PRAET J, et al. Kidney disease caused by dysregulation of the complement alternative pathway: an etiologic approach[J]. J Am Soc Nephrol, 2015, 26(12):2917-2929. |
| [4] | ZIPFEL P F, WIECH T, STEA E D, et al. CFHR gene variations provide insights in the pathogenesis of the kidney diseases atypical hemolytic uremic syndrome and C3 glomerulopathy[J]. J Am Soc Nephrol, 2020, 31(2):241-256. |
| [5] | LEMAIRE M, NOONE D, LAPEYRAQUE A L, et al. Inherited kidney complement diseases[J]. Clin J Am Soc Nephrol, 2021, 16(6):942-956. |
| [6] | BARBOUR T D, PICKERING M C, TERENCE COOK H. Dense deposit disease and C3 glomerulopathy[J]. Semin Nephrol, 2013, 33(6):493-507. |
| [7] | 车丽双, 林威远. C3肾小球病的诊治进展[J]. 慢性病学杂志, 2022, 23(07):1040-1042. |
| CHE L S, LIN W Y. Progress in the diagnosis and treatment of C3 glomerulopathy[J]. Chronic Pathematology J, 2022, 23(07):1040-1042. | |
| [8] | BOMBACK A S, SANTORIELLO D, AVASARE R S, et al. C3 glomerulonephritis and dense deposit disease share a similar disease course in a large United States cohort of patients with C3 glomerulopathy[J]. Kidney Int, 2018, 93(4):977-985. |
| [9] | MEDJERAL-THOMAS N R, O'SHAUGHNESSY M M, O'REGAN J A, et al. C3 glomerulopathy: clinicopathologic features and predictors of outcome[J]. Clin J Am Soc Nephrol, 2014, 9(1):46-53. |
| [10] | SERVAIS A, NOËL L H, ROUMENINA L T, et al. Acquired and genetic complement abnormalities play a critical role in dense deposit disease and other C3 glomerulopathies[J]. Kidney Int, 2012, 82(4):454-464. |
| [11] | HOU J, REN K Y M, HAAS M. C3 glomerulopathy: a review with emphasis on ultrastructural features[J]. Glomerular Dis, 2022, 2(3):107-120. |
| [12] | NIEPOLSKI L, CZEKAŁA A, SEGET-DUBANIEWICZ M, et al. Diagnostic problems in C3 glomerulopathy[J]. Biomedicines, 2023, 11(4):1101. |
| [13] | 魏瑾莹, 黄瑶, 袁曙光, 等. C3沉积为主的肾小球肾炎52例临床与病理特征[J]. 中南大学学报(医学版), 2024, 49(1):75-83. |
| WEI J Y, HUANG Y, YUAN S G, et al. Clinical and pathological characteristics of 52 cases of glomerulonephritis with C3 deposition as the main component[J]. J Cent South Univ (Med Sci), 2024, 49(1):75-83. | |
| [14] | PICKERING M C, D'AGATI V D, NESTER C M, et al. C3 glomerulopathy: consensus report[J]. Kidney Int, 2013, 84(6):1079-1089. |
| [15] | PıNARBAŞı A S, DURSUN I, GOKCE I, et al. Predictors of poor kidney outcome in children with C3 glomerulopathy[J]. Pediatr Nephrol, 2021, 36(5):1195-1205. |
| [16] | SMITH R J H, APPEL G B, BLOM A M, et al. C3 glomerulopathy - understanding a rare complement-driven renal disease[J]. Nat Rev Nephrol, 2019, 15(3):129-143. |
| [17] | ANDERS H J, KITCHING A R, LEUNG N, et al. Glomerulonephritis: immunopathogenesis and immunotherapy[J]. Nat Rev Immunol, 2023, 23(7):453-471. |
| [18] |
LAFAYETTE R A, CHARU V. Expert discussion on challenges in C3G diagnosis: a podcast article on best practices in kidney biopsies[J]. Adv Ther, 2023, 40(12):5557-5566.
doi: 10.1007/s12325-023-02654-3 pmid: 37751024 |
| [19] | VISWANATHAN G K, NADA R, KUMAR A, et al. Clinico-pathologic spectrum of C3 glomerulopathy-an Indian experience[J]. Diagn Pathol, 2015, 10:6. |
| [20] | HOU J, MARKOWITZ G S, BOMBACK A S, et al. Toward a working definition of C3 glomerulopathy by immunofluorescence[J]. Kidney Int, 2014, 85(2):450-456. |
| [1] | 徐图, 史春桃, 韩玮, 姚丽倩, 陈超波, 房灵, 顾婷婷. 乳腺癌组织中Survivin与TK1的协同表达现象及临床意义[J]. 诊断学理论与实践, 2025, 24(05): 518-528. |
| [2] | 杨梅, 廖啟安, 谭全会, 李婷婷, 张毅, 陈洁, 汤正好. 医院获得性细菌性脑膜炎患者预后不良的危险因素分析及列线图预测模型的构建[J]. 诊断学理论与实践, 2025, 24(04): 441-448. |
| [3] | 吴双成, 郁胜强. 2025版KDIGO常染色体显性多囊肾病评估、管理和治疗临床实践指南要点解读[J]. 诊断学理论与实践, 2025, 24(03): 255-262. |
| [4] | 周晓蝶, 戚荣鑫, 王璇, 余波, 王建军, 石群立, 饶秋, 鲍炜. 尿路上皮癌PD-L1、AR及P53表达及其与临床预后相关性[J]. 诊断学理论与实践, 2025, 24(03): 286-292. |
| [5] | 李卓含, 黄新韵, 郭睿, 易红梅, 许彭鹏, 武志芳, 李彪. 滤泡合并弥漫大B细胞淋巴瘤的PET/CT特征及其联合IPI在预后评估中的价值[J]. 诊断学理论与实践, 2025, 24(02): 178-186. |
| [6] | 阮淼, 笪倩, 许海敏, 董磊, 费晓春. HER2低表达乳腺癌临床病理学特征及预后研究[J]. 诊断学理论与实践, 2024, 23(05): 500-508. |
| [7] | 王玉蓉, 汪元元, 翁海燕. 胃肠道平滑肌肉瘤临床病理分析3例报告[J]. 诊断学理论与实践, 2024, 23(05): 537-541. |
| [8] | 李卓含, 黄新韵, 郭睿, 李彪. 18F-FDG PET/CT在滤泡性淋巴瘤诊断和预后评估中的研究进展[J]. 诊断学理论与实践, 2024, 23(04): 439-444. |
| [9] | 朱维维, 李倩, 吴凡, 翟志敏. 100例骨髓增生异常性肿瘤患者基因突变及其与临床特征间的关系[J]. 诊断学理论与实践, 2024, 23(03): 305-312. |
| [10] | 王书奎, 顾心亮. tsRNA作为肿瘤诊断和预后标志物的研究进展[J]. 诊断学理论与实践, 2023, 22(05): 413-420. |
| [11] | 李一林, 陈杨, 李艳艳, 冯旭娇, 章程, 李健, 沈琳. 循环肿瘤细胞检测在常见恶性肿瘤精准医学中的应用和展望[J]. 诊断学理论与实践, 2023, 22(04): 332-340. |
| [12] | 刘英婷, 易红梅, 王雪, 杨春雪, 欧阳斌燊, 许海敏, 王朝夫. 十二指肠型滤泡性淋巴瘤17例临床病理特征及预后分析[J]. 诊断学理论与实践, 2023, 22(04): 362-368. |
| [13] | 张兰兰, 杨巧, 聂尊珍, 郭英. 胸膜SMARCA4缺失未分化肿瘤1例报告[J]. 诊断学理论与实践, 2023, 22(04): 389-392. |
| [14] | 胡静静, 沈银忠, 刘莉, 卢洪洲. 艾滋病合并播散性非结核分枝杆菌病诊治现状及研究进展[J]. 诊断学理论与实践, 2023, 22(04): 402-406. |
| [15] | 徐莉, 高华杰, 杨梦歌, 李悦, 季苏琼. 合并抗TRIM21/Ro52抗体阳性的抗SRP阳性坏死性肌病患者临床特点分析[J]. 诊断学理论与实践, 2023, 22(03): 247-254. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||