诊断学理论与实践 ›› 2025, Vol. 24 ›› Issue (02): 155-162.doi: 10.16150/j.1671-2870.2025.02.006
常蕊, 李纪强, 杨琰昭, 柴维敏, 严福华, 董海鹏( )
)
收稿日期:2025-01-07
接受日期:2025-03-08
出版日期:2025-04-25
发布日期:2025-07-11
通讯作者:
董海鹏 E-mail:dhp40427@rjh.com.cn
CHANG Rui, LI Jiqiang, YANG Yanzhao, CHAI Weimin, YAN Fuhua, DONG Haipeng.()
Received:2025-01-07
Accepted:2025-03-08
Published:2025-04-25
Online:2025-07-11
摘要:
目的: 评估基于光子计数CT(photon-counting computed tomography, PCCT)的胰腺低剂量动态容积灌注CT(volume perfusion computed tomography, VPCT)扫描中单期图像的图像质量及其对胰腺导管腺癌(pancreatic ductal adenocarcinoma, PDAC)进行形态学评估的可行性。 方法: 2024年4月至8月,前瞻性收集疑似PDAC的患者,术前行胰腺VPCT扫描,纳入经组织病理学确诊为PDAC的55例患者,记录并计算检查辐射剂量。分析灌注时间衰减曲线,分别基于T3D、55 keV和70 keV虚拟单能量图像(virtual monoenergetic image, VMI),提取最佳胰腺实质期和门静脉期单期图像,用于临床诊断和PDAC的形态学评估。对图像进行主观评分,并测量图像中病灶、正常胰腺实质、胰周血管及腹壁脂肪CT值,以腹壁脂肪CT值标准差为图像噪声值,计算病灶、正常胰腺实质、胰周血管信噪比以及病灶、胰周血管对比噪声比(contrast-to-noise ratio, CNR)。采用Cohen’s kappa系数评估观察者主观评价一致性,采用单因素重复测量方差分析和Friedman H检验对各组图像定量评价指标及主观评分进行比较。 结果: VPCT扫描平均有效辐射剂量为(18.0 ± 4.9) mSv。基于重建图像提取的胰腺实质期和门静脉期单期图像均符合临床诊断质量标准,图像主观质量评分均≥3分。55 keV VMI重建图像提取的胰腺实质期单期图像中,PDAC病灶CNR为11.1±4.4,T3D为9.1±3.7,70 keV VMI为8.0±3.2;门静脉期55 keV VMI中,PDAC病灶CNR为6.3±3.0,T3D为5.7±3.0,而70 keV VMI为4.9±2.7。55 keV VMI重建提取单期图像表现出最高PDAC病灶CNR(P<0.001),表现出最高正常胰腺实质和胰周血管信噪比、胰周血管CNR,以及最佳PDAC病灶对比度主观评分。55 keV VMI和T3D重建单期图像的图像噪声[胰腺实质期(8.3±2.1)比(8.2±2.1),门静脉期(8.4±2.1)比(8.3±2.2)]差异无统计学意义(P=0.599、0.683),两者的图像噪声均高于70 keV VMI(胰腺实质期7.1±1.9,门静脉期7.3±1.8)(P<0.001)。 结论: 基于PCCT低剂量胰腺动态VPCT成像方案所获得的灌注扫描单期图像,可用于PDAC成像及形态学评估,55 keV VMI重建能够进一步优化PDAC的图像质量。
中图分类号:
常蕊, 李纪强, 杨琰昭, 柴维敏, 严福华, 董海鹏. 光子计数CT胰腺低剂量动态容积灌注扫描中单期图像对胰腺癌图像的评估价值[J]. 诊断学理论与实践, 2025, 24(02): 155-162.
CHANG Rui, LI Jiqiang, YANG Yanzhao, CHAI Weimin, YAN Fuhua, DONG Haipeng.. Evaluation value of single-phase images from photon-counting CT-based low-dose pancreatic dynamic volume perfusion scanning for pancreatic cancer imaging[J]. Journal of Diagnostics Concepts & Practice, 2025, 24(02): 155-162.
表1
光子计数CT胰腺动态容积灌注图像采集及重建参数
| Acquisition parameters Parameter | |
|---|---|
| Scan mode | PCCT(NAEOTOM Alpha) |
| Tube voltage (kVp) | 90 |
| Image quality (IQ) level | 80 |
| Tube current | Care Dose 4D |
| Spiral pitch | 1.0 |
| Rotation time(s) | 0.25 |
| Collimation(mm) | 144 × 0.4 |
| Total acquisition time(s) | 47(began at 7) |
| Z-axis coverage *(cm) | 16 - 25 |
| Number of scan cycles † | 17 - 23 |
| Contrast Volume(mL) | 40 |
| Iodine concentration(mg/mL) | 400 |
| Flow rate(mL/s) | 4 |
| Reconstruction Parameters | |
| Quantum iterative reconstruction | QIR 4 |
| Reconstruction filter kernel | Br 40 |
| Slice thickness and increment (mm) | 1 / 1 |
| Image reconstruction | 55 keV / 70 keV / T3D |
图1
光子计数CT VPCT扫描单期图像提取A:经自动运动校正及4D噪声抑制技术进行图像自动化处理后,在正常胰腺实质及门静脉主干腔内手动放置ROI。B:生成灌注时间衰减曲线。在灌注图像采集序列中,第一个扫描周期的图像作为平扫图像使用,而胰腺实质和门静脉在时间衰减曲线曲线中强化峰值时间点的图像则被手动选定为胰腺实质期和门静脉期的灌注单期图像,用于常规临床诊断与形态学评估。C-E:胰腺尾部PDAC患者,基于55 keV VMI重建图像所获取的灌注单期图像。C为平扫,D为胰腺实质期,E为门静脉期。
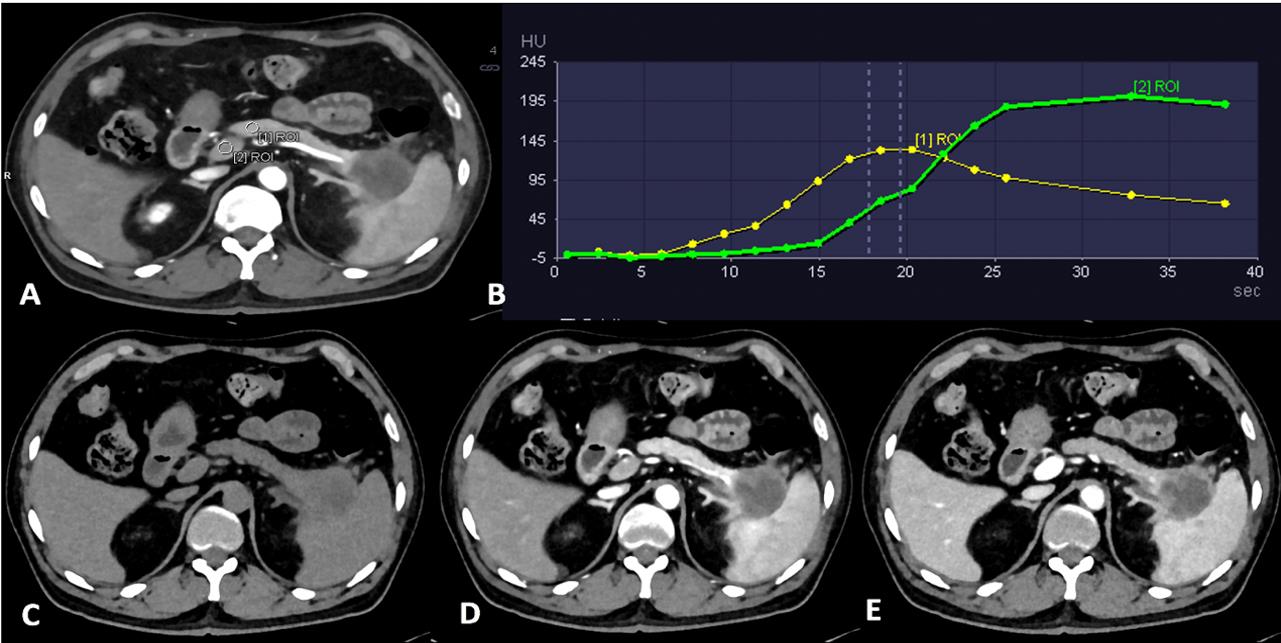
表2
研究人群一般资料及辐射剂量
| Parameter | Value |
|---|---|
| Sex | Male 34,Female 21 |
| Age(y) | 66.4 ± 6.6 (49-78) |
| Weight(kg) | 62.5 ± 10.2 (40-83) |
| Height(m) | 1.66 ± 0.90 (1.45-1.86) |
| BMI(kg/m2) | 22.7 ± 3.2 (17.6-32.9) |
| Z-axis range(cm) | 18.7 ± 2.2 (16-25) |
| No. of scan cycles | 20 ± 2.0 (17-23) |
| CTDIvol(mGy) | 58.7 ± 14.6 (28.3-95.4) |
| DLP(mGy · cm) | 1199.4 ± 328.8 (472.5-1 943.1) |
| ED(mSv) | 18.0 ± 4.9 (7.1-29.2) |

图2
光子计数CT的VPCT扫描单期图像质量主观评分
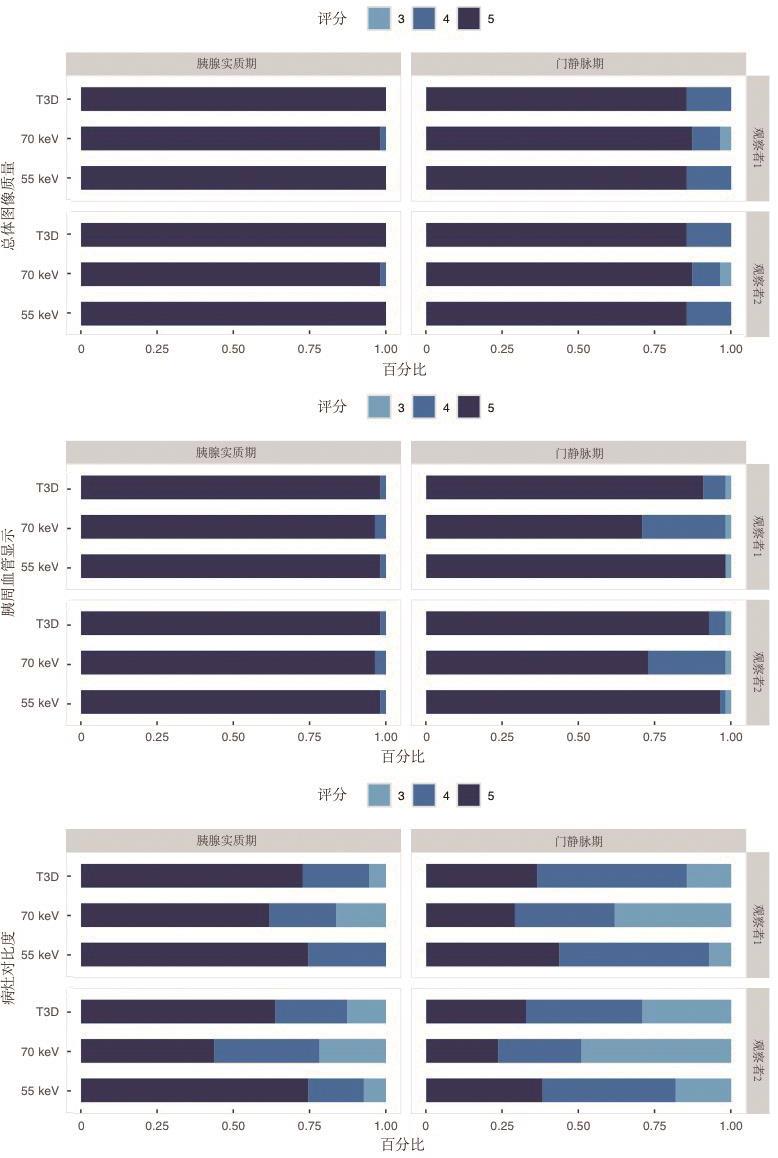
表3
光子计数CT VPCT扫描单期图像质量客观评价
| Item | T3D | 70 keV | 55 keV | P * | P† | P ‡ | P§ |
|---|---|---|---|---|---|---|---|
| Pancreatic parenchymal phase | |||||||
| Image noise (HU) | 8.2 ± 2.1 | 7.1 ± 1.9 | 8.3 ± 2.1 | < 0.001 | < 0.001 | 0.599 | < 0.001 |
| SNR parenchyma | 16.3 ± 5.9 | 16.7 ± 5.0 | 18.8 ± 6.4 | < 0.001 | 0.002 | < 0.001 | < 0.001 |
| SNR vessel | 35.9 ± 15.9 | 36.1 ± 12.5 | 46.8 ± 19.8 | < 0.001 | < 0.001 | < 0.001 | < 0.001 |
| SNR lesion | 7.2 ± 1.8 | 7.5 ± 2.1 | 7.6 ± 2.0 | 0.036 | 0.062 | 0.003 | 0.505 |
| CNR vessel | 27.0 ± 17.7 | 25.7 ± 16.2 | 36.9 ± 23.0 | < 0.001 | < 0.001 | < 0.001 | < 0.001 |
| CNR lesion | 9.1 ± 3.7 | 8.0 ± 3.2 | 11.1 ± 4.4 | < 0.001 | < 0.001 | < 0.001 | < 0.001 |
| Portal venous phase | |||||||
| Image noise (HU) | 8.3 ± 2.2 | 7.3 ± 1.8 | 8.4 ± 2.1 | < 0.001 | < 0.001 | 0.683 | < 0.001 |
| SNR parenchyma | 12.4 ± 3.2 | 11.8 ± 3.2 | 13.3 ± 3.6 | < 0.001 | 0.033 | < 0.001 | < 0.001 |
| SNR vessel | 20.9 ± 6.3 | 18.5 ± 5.0 | 23.3 ± 7.5 | < 0.001 | < 0.001 | < 0.001 | < 0.001 |
| SNR lesion | 6.5 ± 2.0 | 6.7 ± 1.9 | 6.9 ± 2.2 | 0.003 | 0.009 | < 0.001 | 0.231 |
| CNR vessel | 10.6 ± 4.4 | 9.0 ± 3.7 | 13.5 ± 5.7 | < 0.001 | < 0.001 | < 0.001 | < 0.001 |
| CNR lesion | 5.7 ± 3.0 | 4.9 ± 2.7 | 6.3 ± 3.0 | < 0.001 | < 0.001 | < 0.001 | < 0.001 |
| [1] | LI H O, SUN C, XU Z D, et al. B. Low-dose whole organ CT perfusion of the pancreas: preliminary study[J]. Abdom Imaging,2014,39(1):40-7. |
| [2] |
O'MALLEY R B, SOLOFF E V, COVELER A L, et al. Feasibility of wide detector CT perfusion imaging performed during routine staging and restaging of pancreatic ductal adenocarcinoma[J]. Abdom Radiol (NY),2021,46(5):1992-2002.
doi: 10.1007/s00261-020-02786-y pmid: 33079256 |
| [3] |
O'MALLEY R B, COX D, SOLOFF E V, et al. CT perfusion as a potential biomarker for pancreatic ductal adenocarcinoma during routine staging and restaging[J]. Abdom Radiol (NY),2022,47(11):3770-3781.
doi: 10.1007/s00261-022-03638-7 pmid: 35972550 |
| [4] | PERIK T H, VAN GENUGTEN E A J, AARNTZEN E H J G, et al. Quantitative CT perfusion imaging in patients with pancreatic cancer: a systematic review[J]. Abdom Radiol (NY),2022,47(9):3101-3117. |
| [5] | SKORNITZKE S, VATS N, MAYER P, et al. Pancreatic CT perfusion: quantitative meta-analysis of disease discrimination, protocol development, and effect of CT parameters[J]. Insights Imaging,2023,14(1):132. |
| [6] |
HAMDY A, ICHIKAWA Y, TOYOMASU Y, et al. Perfusion CT to assess response to neoadjuvant chemotherapy and radiation therapy in pancreatic ductal adenocarcinoma: initial experience[J]. Radiology,2019,292(3):628-635.
doi: 10.1148/radiol.2019182561 pmid: 31287389 |
| [7] | WANG X, HENZLER T, GAWLITZA J, et al. Image qua-lity of mean temporal arterial and mean temporal portal venous phase images calculated from low dose dynamic volume perfusion CT datasets in patients with hepatocellular carcinoma and pancreatic cancer[J]. Eur J Radiol,2016,85(11):2104-2110. |
| [8] |
WILLEMINK M J, PERSSON M, POURMORTEZA A, et al. Photon-counting CT: technical principles and clinical prospects[J]. Radiology,2018,289:293-312
doi: 10.1148/radiol.2018172656 pmid: 30179101 |
| [9] |
FLOHR T, SCHMIDT B. Technical basics and clinical benefits of photon-counting CT[J]. Invest Radiol,2023,58:441-450
doi: 10.1097/RLI.0000000000000980 pmid: 37185302 |
| [10] |
LI J, CHEN X Y, XU K, et al. Detection of insulinoma: one-stop pancreatic perfusion CT with calculated mean temporal images can replace the combination of bi-phasic plus perfusion scan[J]. Eur Radiol,2020,30(8):4164-4174.
doi: 10.1007/s00330-020-06657-4 pmid: 32189051 |
| [11] | MICHALSKI C W, ERKAN M, HUSER N, et al. Resection of primary pancreatic cancer and liver metastasis: a systematic review[J]. Dig Surg,2008,25(6):473–480 |
| [12] | KLEIN F, PUHL G, GUCKELBERGER O, et al. The impact of simultaneous liver resection for occult liver metastases of pancreatic adenocarcinoma[J]. Gastroenterol Res Pract,2012(6):939-950 |
| [13] | LENG S, BRUESEWITZ M, TAO S, et al. Photon-coun-ting detector CT: system design and clinical applications of an emerging technology[J]. Radiographics,2019,39(3):729-743. |
| [14] |
KIM J, MABUD T, HUANG C, et al. Inter-reader agreement of pancreatic adenocarcinoma resectability assessment with photon counting versus energy integrating detector CT[J]. Abdom Radiol (NY),2024,49(9):3149-3157.
doi: 10.1007/s00261-024-04298-5 pmid: 38630314 |
| [15] | 谢环环, 林晓珠, 王晴柔, 等. CT能谱成像在胰腺癌病灶显示中的应用价值[J].实用放射学杂志,2017,33(5):750-753. |
| XIE H H, LIN X Z, WANG Q R, et al. Value of CT spectral imaging in demonstration of pancreatic ductal adenocarcinoma[J]. J Pract Radiol, 2017, 33(5):750-753. | |
| [16] | BEER L, TOEPKER M, BA-SALAMAH A, et al. Objective and subjective comparison of virtual monoenergetic vs. polychromatic images in patients with pancreatic ductal adenocarcinoma[J]. Eur Radiol,2019,29(7):3617-3625. |
| [17] | 杨琰昭, 常蕊, 王晴柔, 等. 双层探测器光谱CT虚拟单能量图像在胰腺导管腺癌术前评估中的优化研究[J]. 上海交通大学学报:医学版, 2022, 42(9):1323-1328. |
| YANG Y Z, CHANG R, WANG Q R, et al. Optimized study of virtual monoenergetic images derived from a dual-layer spectral detector CT in the preoperative evalua-tion of pancreatic ductal adenocarcinoma[J]. J Shanghai Jiaotong Univ(Med Sci),2022,(9):1323-1328 | |
| [18] | DECKER J A, BECKER J, HARTING M, et al. Optimal conspicuity of pancreatic ductal adenocarcinoma in virtual monochromatic imaging reconstructions on a photon-counting detector CT: comparison to conventional MDCT[J]. Abdom Radiol (NY),2024,49(1):103-116. |
| [1] | 吕海英, 陆勇, 贺娜英. 光子计数CT在神经系统成像中的临床价值[J]. 诊断学理论与实践, 2025, 24(02): 212-219. |
| [2] | 周山税, 秦乐, 常蕊, 杜联军, 严福华, 刘方韬. 基于光子计数探测器CT能谱定位像定量评估股骨颈骨密度的前瞻性研究[J]. 诊断学理论与实践, 2025, 24(02): 163-169. |
| [3] | 蔡欣欣, 邓嵘, 徐欣欣, 许芷涵, 常蕊, 董海鹏, 林慧敏, 严福华. 基于光子计数CT的肝脏脂肪分数定量测定与磁共振质子密度脂肪分数间的一致性研究[J]. 诊断学理论与实践, 2025, 24(02): 146-154. |
| [4] | 王梦真, 鲍守钰, 刘鹏, 严福华, 杨文洁. 光子计数CT在心血管疾病中的应用[J]. 诊断学理论与实践, 2025, 24(02): 125-134. |
| [5] | 李卫侠, 严福华. 光子计数CT在肝脏疾病中的应用进展[J]. 诊断学理论与实践, 2025, 24(02): 118-124. |
| [6] | 黄瑞坤, 杨琰昭, 柴维敏. 光子计数CT在胰腺成像中的应用进展[J]. 诊断学理论与实践, 2025, 24(02): 111-117. |
| [7] | 吕晓宇, 冯威铭, 周慧赟, 李纪强, 董海鹏, 黄娟. 基于磁共振深度学习重建算法缩短扫描时间的可行性分析:水模研究[J]. 诊断学理论与实践, 2024, 23(02): 131-138. |
| [8] | 范婧, 杨文洁, 王梦真, 陆伟, 石骁萌, 朱宏. 深度学习重建算法在低管电压冠状动脉CT血管成像中的应用[J]. 诊断学理论与实践, 2022, 21(03): 374-379. |
| [9] | 张雪坤, 李彦, 严福华, 赵洪飞, 宋琦. 基于光梭成像的新型加速技术在颅脑MRI中的应用价值研究[J]. 诊断学理论与实践, 2021, 20(04): 378-383. |
| [10] | 常蕊, 杨琰昭, 孔德艳, 徐嘉旭, 曹琪琪, 杨文洁, 严福华, 董海鹏. 不同管电压、管电流扫描方案联合KARL迭代重建在新型冠状病毒肺炎疫情期间胸部CT筛查中的应用研究[J]. 诊断学理论与实践, 2020, 19(02): 182-187. |
| [11] | 方姝, 杜联军, 秦乐, 董海鹏, 严福华, 王韬. 腰椎间盘低剂量CT扫描结合迭代模型重建的图像质量及诊断效能的研究[J]. 诊断学理论与实践, 2019, 18(03): 344-348. |
| [12] | 胡蒙, 朱怀仕, 宋琦. 口腔种植定位术前评估中颌骨低剂量多层螺旋CT检查的应用[J]. 诊断学理论与实践, 2018, 17(01): 66-69. |
| [13] | 王韬, 傅萌, 肖瑞杰, 董海鹏, 李若坤, 严福华. Multivane XD技术在肝脏T2WI成像中的应用价值[J]. 诊断学理论与实践, 2016, 15(05): 521-524. |
| [14] | 刘欢欢, 张欢, 石磊, 潘自来, 李向亭, 杜联军, 丁蓓, 宋琦, 凌华威, 陈克敏, 严福华,. 第二代双源CT双能量虚拟平扫在直肠癌诊断中的应用评估[J]. 诊断学理论与实践, 2013, 12(02): 216-220. |
| [15] | 石磊, 张欢, 潘自来, 刘欢欢, 李向亭, 杜联军, 丁蓓, 宋琦, 凌华威, 刘博, 陈克敏, 严福华,. 胃癌双能量CT成像与病理分级的相关性研究[J]. 诊断学理论与实践, 2013, 12(01): 65-69. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||