内科理论与实践 ›› 2022, Vol. 17 ›› Issue (03): 208-213.doi: 10.16138/j.1673-6087.2022.03.007
陈敏, 车在前, 陈影, 马丽, 赵冰, 周伟君, 毛恩强, 陈尔真
收稿日期:2021-10-13
出版日期:2022-05-30
发布日期:2022-08-09
通讯作者:
周伟君
基金资助:CHEN Min, CHE Zaiqian, CHEN Ying, MA Li, ZHAO Bing, ZHOU Weijun, MAO Enqiang, CHEN Erzhen
Received:2021-10-13
Online:2022-05-30
Published:2022-08-09
Contact:
ZHOU Weijun
摘要:
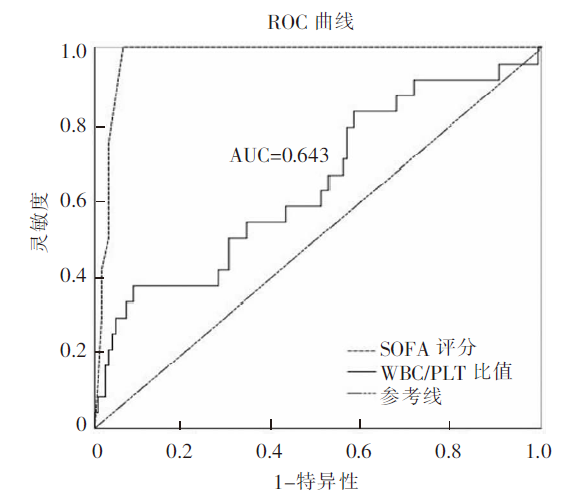
目的:探讨白细胞和血小板(white blood cell/platelet, WBC/PLT)比值对脓毒症预后早期评估中的临床价值和相关影响因素。方法:前瞻性分析2018年6月至2020年6月上海交通大学医学院附属瑞金医院急诊重症监护室(emergency intensive care unit, EICU)收治的150例脓毒症患者临床资料。根据预后分为存活组和死亡组,比较2组患者发病后24 h内WBC/PLT比值及临床生化指标差异。WBC/PLT比值与脓毒症患者各危险因素的相关性采用Pearson相关分析。采用Cox风险回归模型分析患者预后的影响因素,并绘制受试者工作特征曲线(receiver operating characteristic curve,ROC曲线)评估WBC/PLT比值对死亡的预测效果。结果:150例患者中存活组126例,死亡组24例,2组脓毒症患者年龄、性别、感染类型和基础疾病构成比差异无统计学意义(均P>0.05);死亡组脓毒症休克比例、使用血管活性药物和机械通气及血液净化比例显著高于存活组(均P<0.05);死亡组降钙素原、尿素氮、天冬氨酸转氨酶、凝血酶原时间、纤维蛋白降解产物、D-二聚体、前脑钠肽以及序贯器官衰竭评估(sequential organ failure assessment,SOFA)评分显著高于存活组(均P<0.05);脓毒症死亡组患者WBC/PLT比值(0.56±1.27)显著高于存活组(0.15±0.42)(P<0.05)。150例研究对象Pearson相关分析显示:WBC/PLT比值与C反应蛋白、降钙素原、尿素氮、肌酐、前脑钠肽、活化部分凝血酶原时间、纤维蛋白降解产物、D-二聚体呈正相关,随之增加而增加(P<0.05)。Cox回归模型分析显示,高WBC/PLT比值、高尿素氮水平、高SOFA评分为影响脓毒症患者预后的独立危险因素(P<0.05),ROC曲线分析显示,WBC/PLT比值对脓毒症患者预后有预测价值,曲线下面积为0.643[95%置信区间(confidence interval,CI):0.516~0.770,P=0.026],最佳截断值为0.186,灵敏度为37.5%,特异度为91.3%。结论:WBC/PLT比值用于脓毒症病情评估特异性较高,可以早期预估患者的预后,值得临床推广应用。
中图分类号:
陈敏, 车在前, 陈影, 马丽, 赵冰, 周伟君, 毛恩强, 陈尔真. 白细胞血小板比值早期评估脓毒症预后的临床研究[J]. 内科理论与实践, 2022, 17(03): 208-213.
CHEN Min, CHE Zaiqian, CHEN Ying, MA Li, ZHAO Bing, ZHOU Weijun, MAO Enqiang, CHEN Erzhen. Clinical study of leukocyte-to-platelet ratio in early evaluating prognosis of sepsis[J]. Journal of Internal Medicine Concepts & Practice, 2022, 17(03): 208-213.
表1
脓毒症患者存活组和死亡组的一般临床资料比较[$\bar{x}\pm s$/n(%)]
| 一般资料 | 存活组(n=126) | 死亡组(n=24) | t或χ2 | P |
|---|---|---|---|---|
| 年龄(岁) | 52.1±15.7 | 63.5±18.1 | -3.161 | 0.685 |
| 男性 | 71(56.3) | 10(41.7) | 1.750 | 0.186 |
| 脓毒症休克 | 14(11.1) | 16(66.7) | 29.630 | 0.000 |
| 感染部位 | 3.684 | 0.298 | ||
| 肺 | 53(42.1) | 10(41.7) | ||
| 泌尿道 | 50(39.7) | 9(37.5) | ||
| 胆道 | 21(16.7) | 3(12.5) | ||
| 其他 | 2(1.6) | 2(8.3) | ||
| 基础疾病 | 1.779 | 0.619 | ||
| 无 | 26(20.6) | 5(20.8) | ||
| 糖尿病 | 44(34.9) | 10(41.7) | ||
| 高血压 | 14(11.1) | 4(16.7) | ||
| 高脂血症 | 42(33.3) | 5(20.8) | ||
| 收缩压(mmHg) | 125.0±25.8 | 126.5±27.1 | -0.240 | 0.911 |
| 舒张压(mmHg) | 81.5±20.8 | 72.2±17.7 | 2.045 | 0.076 |
| 心率(次/min) | 89.3±23.5 | 108.8±22.0 | -3.768 | 0.601 |
| 氧合指数 | 372.5±180.9 | 115.8±48.7 | 21.276 | 0.000 |
| 血管活性药物 | 14(11.1) | 16(66.7) | 29.630 | 0.000 |
| 机械通气 | 32(25.4) | 18(75.0) | 22.321 | 0.000 |
| 血液净化 | 21(16.7) | 10(41.7) | 7.789 | 0.020 |
| 住院天数(d) | 36.8±33.8 | 16.8±15.5 | 5.037 | 0.026 |
表2
脓毒症患者存活组和死亡组治疗前实验室检测指标比较($\bar{x}\pm s$)
| 实验室检查 | 存活组 (n=126) | 死亡组 (n=24) | t | P |
|---|---|---|---|---|
| WBC计数(×109/L) | 12.9±7.5 | 14.6±7.5 | -0.946 | 0.382 |
| PLT计数(×109/L) | 166.5±96.7 | 140.7±112.8 | 1.163 | 0.068 |
| CRP(mg/L) | 8.3±4.8 | 17.5±9.3 | -3.915 | 0.207 |
| PCT(mg/L) | 6.4±2.2 | 25.7±9.1 | -3.030 | 0.000 |
| 空腹血糖(mmol/L) | 9.9±4.7 | 11.6±5.6 | -1.495 | 0.148 |
| 尿素氮(mmol/L) | 9.1±8.8 | 21.4±16.7 | -5.310 | 0.000 |
| 肌酐(μmol/L) | 121.4±81.1 | 205.6±141.0 | -2.135 | 0.404 |
| ALT(U/L) | 60.6±37.4 | 71.0±39.9 | -0.340 | 0.430 |
| AST(U/L) | 75.9±65.3 | 216.9±91.3 | -2.270 | 0.000 |
| APTT(s) | 32.7±5.9 | 36.1±7.6 | -2.159 | 0.211 |
| PT(s) | 14.1±2.4 | 15.5±4.3 | -1.898 | 0.018 |
| FDP(g/L) | 21.7±4.9 | 38.9±8.4 | -2.354 | 0.003 |
| D-二聚体(mg/L) | 7.1±6.1 | 13.7±4.2 | -2.447 | 0.001 |
| pro-BNP(mg/L) | 2.0±0.6 | 11.1±1.4 | -5.315 | 0.000 |
| cTnI(μg/L) | 1.1±0.3 | 2.1±1.1 | -1.166 | 0.205 |
| 乳酸(mmol/L) | 2.9±2.4 | 3.7±3.2 | -0.516 | 0.223 |
表3
WBC/PLT比值与脓毒症患者一般资料及实验室检测指标的Pearson相关性分析
| 项目 | r | P |
|---|---|---|
| 年龄 | 0.150 | 0.068 |
| 性别 | 0.108 | 0.188 |
| 收缩压 | -0.078 | 0.341 |
| 舒张压 | -0.046 | 0.574 |
| 心率 | 0.151 | 0.066 |
| 氧合指数 | -0.146 | 0.157 |
| CRP | 0.220 | 0.007 |
| PCT | 0.457 | 0.000 |
| 空腹血糖 | 0.126 | 0.137 |
| 尿素氮 | 0.389 | 0.000 |
| 肌酐 | 0.188 | 0.021 |
| ALT | 0.020 | 0.806 |
| AST | 0.001 | 0.994 |
| pro-BNP | 0.370 | 0.000 |
| cTnI | 0.096 | 0.245 |
| APTT | 0.240 | 0.034 |
| PT | 0.213 | 0.061 |
| FDP | 0.243 | 0.032 |
| D-二聚体 | 0.252 | 0.026 |
| 乳酸 | 0.105 | 0.611 |
表4
影响脓毒症患者预后相关因素的Cox回归模型分析
| 相关因素 | β | SE | Wald | OR | 95%CI | P |
|---|---|---|---|---|---|---|
| WBC/PLT比值 | 0.413 | 0.200 | 4.253 | 1.511 | 1.021~2.236 | 0.039 |
| 尿素氮 | 0.024 | 0.012 | 3.909 | 1.024 | 1.000~1.048 | 0.048 |
| SOFA评分 | 0.272 | 0.047 | 33.417 | 1.312 | 1.197~1.439 | 0.000 |
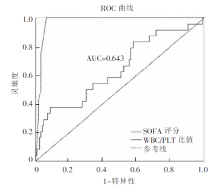
图1
WBC/PLT比值和SOFA评分对脓毒症患者死亡风险预测的ROC曲线
| [1] |
Weng L, Zeng XY, Yin P, et al. Sepsis-related mortality in China: a descriptive analysis[J]. Intensive Care Med, 2018, 44(7): 1071-1080.
doi: 10.1007/s00134-018-5203-z pmid: 29846748 |
| [2] |
Xie J, Wang H, Kang Y, et al. The epidemiology of sepsis in Chinese ICUs[J]. Crit Care Med, 2020, 48(3): e209-e218.
doi: 10.1097/CCM.0000000000004155 URL |
| [3] |
Kaukonen KM, Bailey M, Suzuki S, et al. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000-2012[J]. JAMA, 2014, 311(13): 1308-1316.
doi: 10.1001/jama.2014.2637 URL |
| [4] |
Rhodes A, Phillips G, Beale R, et al. The surviving sepsis campaign bundles and outcome: results from the International Multicentre Prevalence Study on Sepsis (the IMPreSS study)[J]. Intensive Care Med, 2015, 41(9): 1620-1628.
doi: 10.1007/s00134-015-3906-y URL |
| [5] |
Fleischmann C, Scherag A, Adhikari NK, et al. Assessment of Global Incidence and Mortality of Hospital-treated Sepsis. Current Estimates and Limitations[J]. Am J Respir Crit Care Med, 2016, 193(3): 259-272.
doi: 10.1164/rccm.201504-0781OC URL |
| [6] |
Larsen FF, Petersen JA. Novel biomarkers for sepsis: a narrative review[J]. Eur J Intern Med, 2017, 45: 46-50.
doi: 10.1016/j.ejim.2017.09.030 URL |
| [7] | Giannakopoulos K, Hoffmann U, Ansari U, et al. The use of biomarkers in sepsis[J]. Curr Pharm Biotechnol, 2017, 18(6): 499-507. |
| [8] |
Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of clinical criteria for sepsis: for the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3)[J]. JAMA, 2016, 315(8): 762-774.
doi: 10.1001/jama.2016.0288 URL |
| [9] |
Churpek MM, Snyder A, Han X, et al. Quick sepsis-related organ failure assessment, systemic inflammatory response syndrome, and early warning scores for detecting clinical deterioration in infected patients outside the intensive care unit[J]. Am J Respir Crit Care Med, 2017, 195(7): 906-911.
doi: 10.1164/rccm.201604-0854OC URL |
| [10] |
Martin JB, Badeaux JE. Interpreting laboratory tests in infection: making sense of biomarkers in sepsis and systemic inflammatory response syndrome for intensive care unit patients[J]. Crit Care Nurs Clin North Am, 2017, 29(1): 119-130.
doi: 10.1016/j.cnc.2016.09.004 URL |
| [11] | Scarlatescu E, Tomescu D, Arama SS. Anticoagulant therapy in sepsis[J]. J Crit Care Med (Targu Mures), 2017, 3(2): 63-69. |
| [12] |
Simmons J, Pittet JF. The coagulopathy of acute sepsis[J]. Curr Opin Anaesthesiol, 2015, 28(2): 227-236.
doi: 10.1097/ACO.0000000000000163 pmid: 25590467 |
| [13] | Yao YM, Luan YY, Zhang QH, et al. Pathophysiological aspects of sepsis[J]. Methods Mol Biol, 2015, 1237: 5-15. |
| [14] |
Schnoor M, García Ponce A, Vadillo E, et al. Actin dynamics in the regulation of endothelial barrier functions and neutrophil recruitment during endotoxemia and sepsis[J]. Cell Mol Life Sci, 2017, 74(11): 1985-1997.
doi: 10.1007/s00018-016-2449-x URL |
| [15] |
Alves-Filho JC, de Freitas A, Spiller F, et al. The role of neutrophils in severe sepsis[J]. Shock, 2008, 30 Suppl 1: 3-9.
doi: 10.1097/SHK.0b013e3181818466 pmid: 18704017 |
| [16] |
Shen XF, Cao K, Jiang JP, et al. Neutrophil dysregulation during sepsis: an overview and update[J]. J Cell Mol Med, 2017, 21(9): 1687-1697.
doi: 10.1111/jcmm.13112 URL |
| [17] |
Venkata C, Kashyap R, Farmer JC, et al. Thrombocytopenia in adult patients with sepsis: incidence, risk factors, and its association with clinical outcome[J]. J Intensive Care, 2013, 1(1): 9.
doi: 10.1186/2052-0492-1-9 URL |
| [18] |
Woth G, Varga A, Ghosh S, et al. Platelet aggregation in severe sepsis[J]. J Thromb Thrombolysis, 2011, 31(1): 6-12.
doi: 10.1007/s11239-010-0486-0 URL |
| [19] |
Vardon-Bounes F, Ruiz S, Gratacap MP, et al. Platelets are critical key players in sepsis[J]. Int J Mol Sci, 2019, 20(14): 3494.
doi: 10.3390/ijms20143494 URL |
| [20] |
Iba T, Levy JH. Inflammation and thrombosis: roles of neutrophils, platelets and endothelial cells and their interactions in thrombus formation during sepsis[J]. J Thromb Haemost, 2018, 16(2): 231-241.
doi: 10.1111/jth.13911 pmid: 29193703 |
| [21] |
de Stoppelaar SF, van 't Veer C, van der Poll T. The role of platelets in sepsis[J]. Thromb Haemost, 2014, 112(4): 666-677.
doi: 10.1160/TH14-02-0126 URL |
| [22] |
Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3)[J]. JAMA, 2016, 315(8): 801-810.
doi: 10.1001/jama.2016.0287 URL |
| [23] |
American College of Chest Physicians/Society of Critical Care Medicine. American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis[J]. Crit Care Med, 1992. 20(6): 864-874.
doi: 10.1097/00003246-199206000-00025 URL |
| [24] |
Levy MM, Fink MP, Marshall JC, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS international sepsis definitions conference[J]. Intensive Care Med, 2003, 29(4): 530-538.
doi: 10.1007/s00134-003-1662-x URL |
| [25] |
Kaukonen KM, Bailey M, Pilcher D, et al. Systemic inflammatory response syndrome criteria in defining severe sepsis[J]. N Engl J Med, 2015, 372(17): 1629-1638.
doi: 10.1056/NEJMoa1415236 URL |
| [26] |
McDonald B, Dunbar M. Platelets and intravascular immunity: guardians of the vascular space during bloodstream infections and sepsis[J]. Front Immunol, 2019, 10: 2400.
doi: 10.3389/fimmu.2019.02400 pmid: 31681291 |
| [27] |
Thiery-Antier N, Binquet C, Vinault S, et al. Is thrombocytopenia an early prognostic marker in septic shock?[J]. Crit Care Med, 2016, 44(4): 764-772.
doi: 10.1097/CCM.0000000000001520 pmid: 26670473 |
| [28] |
Bouadma L, Luyt CE, Tubach F, et al. Use of procalcitonin to reduce patients’ exposure to antibiotics in intensive care units (PRORATA trial): a multicentre randomised controlled trial[J]. Lancet, 2010, 375(9713): 463-474.
doi: 10.1016/S0140-6736(09)61879-1 pmid: 20097417 |
| [29] |
Thomas MR, Storey RF. The role of platelets in inflammation[J]. Thromb Haemost, 2015, 114(3): 449-458.
doi: 10.1160/TH14-12-1067 URL |
| [30] |
Zhang W, Zheng Y, Feng X, et al. Systemic inflammatory response syndrome in Sepsis-3[J]. BMC Infect Dis, 2019, 19(1): 139.
doi: 10.1186/s12879-019-3790-0 pmid: 30744579 |
| [31] |
Donnelly JP, Safford MM, Shapiro NI, et al. Application of the Third International Consensus Definitions for Sepsis (Sepsis-3) Classification[J]. Lancet Infect Dis, 2017, 17(6): 661-670.
doi: S1473-3099(17)30117-2 pmid: 28268067 |
| [1] | 尹彦江, 罗治文, 陈晓, 张业繁, 黄振, 赵宏, 赵建军, 李智宇, 周健国, 蔡建强, 毕新宇. 肝内胆管癌病人肝脏手术切缘与预后的关系[J]. 外科理论与实践, 2022, 27(3): 221-228. |
| [2] | 杨崔燕, 王豪雨, 陈小松, 沈坤炜. 抑癌基因TP53突变状态与三阴性乳腺癌病人预后的研究[J]. 外科理论与实践, 2022, 27(05): 421-428. |
| [3] | 周易, 陈影, 陈尔真. 甲状腺激素对脓毒症脏器功能维护作用的研究进展[J]. 内科理论与实践, 2022, 17(05): 408-412. |
| [4] | 郑毓真, 郑彦俊, 周易, 祁星, 陈薇薇, 史雯, 周伟君, 杨之涛, 陈影, 毛恩强, 陈尔真. 综合性医院674例脓毒症住院患者的回顾性临床分析[J]. 内科理论与实践, 2022, 17(04): 278-282. |
| [5] | 徐娜娜, 吴涛, 寇明坤, 白海. ASXL1基因突变在急性髓系白血病中的研究进展[J]. 内科理论与实践, 2022, 17(04): 353-355. |
| [6] | 程威, 黄雨桦, 王剑, 李幼生. 影响癌性肠梗阻病人预后的多因素分析[J]. 外科理论与实践, 2022, 27(04): 340-345. |
| [7] | 李蕾, 袁菲, 王朝夫, 许海敏, 王婷. 101例壶腹部腺癌临床病理及预后因素分析[J]. 诊断学理论与实践, 2022, 21(03): 355-361. |
| [8] | 李响, 王杨, 葛晓利, 潘曙明. 中药虎杖治疗脓毒症的研究进展[J]. 内科理论与实践, 2022, 17(01): 92-96. |
| [9] | 符国新 王舒舒 何垚 宋晓萌 朱载瓯. 腮腺手术中应用美容切口与 Blair 切口比较的系统评价及 Meta 分析 [J]. 组织工程与重建外科杂志, 2021, 17(6): 532-. |
| [10] | 沐阳, 陈欣. 血浆降钙素原和C反应蛋白对多发伤病人预后评估的价值[J]. 外科理论与实践, 2021, 26(6): 532-536. |
| [11] | 陈曦, 杜鹃. 多发性骨髓瘤预后风险的精准评估[J]. 诊断学理论与实践, 2021, 20(06): 522-528. |
| [12] | 冯国伟, 张晓娟, 郭睿, 关哲, 王越. 治疗前18F-FDG PET/CT显像对结外NK/T细胞淋巴瘤的预后判断价值[J]. 诊断学理论与实践, 2021, 20(06): 533-539. |
| [13] | 梁亚丽, 赵海港, 项广宇. 应激性高血糖比值预测急性缺血性脑卒中患者溶栓治疗后1年不良预后的价值[J]. 诊断学理论与实践, 2021, 20(06): 562-566. |
| [14] | 王虎, 张姣姣, 孙俊楠, 王海嵘. 白介素-6联合CD4+T淋巴细胞百分比对脓毒症患者预后的评估价值[J]. 内科理论与实践, 2021, 16(06): 404-408. |
| [15] | 宋娟, 邢寅, 黄慧, 陆帅, 秦利. 上海市崇明地区中老年人群血白细胞计数与血尿酸水平相关性研究[J]. 内科理论与实践, 2021, 16(06): 413-417. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||