Journal of Diagnostics Concepts & Practice ›› 2023, Vol. 22 ›› Issue (03): 270-276.doi: 10.16150/j.1671-2870.2023.03.10
• Original articles • Previous Articles Next Articles
YANG Qiao1, FU Xin2, WANG Zhe2, LIU Tantan2,3( )
)
Received:2022-11-24
Online:2023-06-25
Published:2023-11-17
CLC Number:
YANG Qiao, FU Xin, WANG Zhe, LIU Tantan. Cytopathologic analysis of thyroid secondary tumors[J]. Journal of Diagnostics Concepts & Practice, 2023, 22(03): 270-276.
Table 1
Clinical datas of patients with secondary thyroid tumors
| Sex | Age (years) | History disease | Ultrasound results | Follow-up (months) | |
|---|---|---|---|---|---|
| 1 | Female | 57 | / | Right, mixed echo region, 1.9cm×1.5cm | 1 |
| 2 | Female | 64 | Small cell carcinoma of the left lung, 2 years and 8 months, cervical lymph node metastasis lasted 6 months | Right, low echo area, 2.4cm×1.4cm | 24 (death) |
| 3 | Female | 56 | Breast cancer, 5 years and 6 months | Isthmus to the right, Low echo area, 1.7cm×1.2cm | 29 |
| 4 | Female | 58 | Breast cancer, eight years and ten months | Right, low echo area, 2.2cm×1.5cm | 18 |
| 5 | Male | 56 | Squamous cell carcinoma of larynx, 1 year | Right, low echo area, 0.9cm×0.8cm | 24 |
| 6 | Male | 68 | Squamous cell carcinoma of the esophagus, 3 years | Right, low echo area, 1.5cm×1.2cm | 60 (death) |
| 7 | Male | 75 | Squamous cell carcinoma of hypopharynx, 4 years and 2 months | Right, low echo area, 3.2cm×3.7cm | 81 |
| 8 | Male | 64 | Squamous cell carcinoma of the trachea, 5 days | Right, low echo area, 2.8cm×2.6cm | 48 |
Table 2
Comparison of cell morphology and immunophenotype between STN and medullary thyroid carcinoma
| Number of cases | Normal follicles in the background | Arrangement mode | Cytological characteristics | Nuclear chromatin | Positive (IHC) | Negative (IHC) | |
|---|---|---|---|---|---|---|---|
| Adenocarci- noma of lung | 1 | Occasionally | Three-dimensional adenoid structure, papillary structure | Large, abundant cytoplasm, visible mucous vacuoles | Obvious nucleolus | CK7、TTF-1、NapsinA | CA125、WT-1、TG、PAX-8 |
| Small cell carci- noma of lung | 1 | Massive necrosis, apoptosis | Clustered,scattered, Mosaic-like | Uniform size, bare nucleus | Pepper salt like, fine granular | Syn、CD56、CgA | CT、TG |
| Breast cancer | 2 | Not seen | Clumps, clusters, scattered | Difference in size, The cytoplasm is medium to abundant with occasional vacuoles | Hyperchromatic nuclei, nucleolus were not obvious | ER、PR、CK7、GATA3 | TTF-1、PAX-8、CT |
| Squamous cell carcinoma | 4 | More or less, Neutrophils visible | Lamellar, nestlike, scattered | Significant size difference, round or fusiform, cytoplasmic keratosis is common | Hyperchromatic nuclei, polygon, irregular nuclear membranes | P63、P40 | TG |
| Medullary thyr- oid carcinoma | 33 | More or less | Single scattered, cell boundaries is unclear | Plasmacytoid, epithelioid, strange giant cell | Pepper salt like, fine granular | Syn、CD56、CgA、CT | TG |
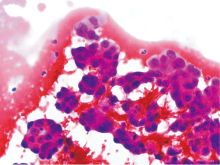
Figure 1
Case 1, metastatic lung adenocarcinoma of thyroid (FNA) Tumor cells form a three-dimensional adenoid or papillary structure, the cells are rich in cytoplasm with large and lightly staining nucleus, distinct nucleoli (HE, ×400).
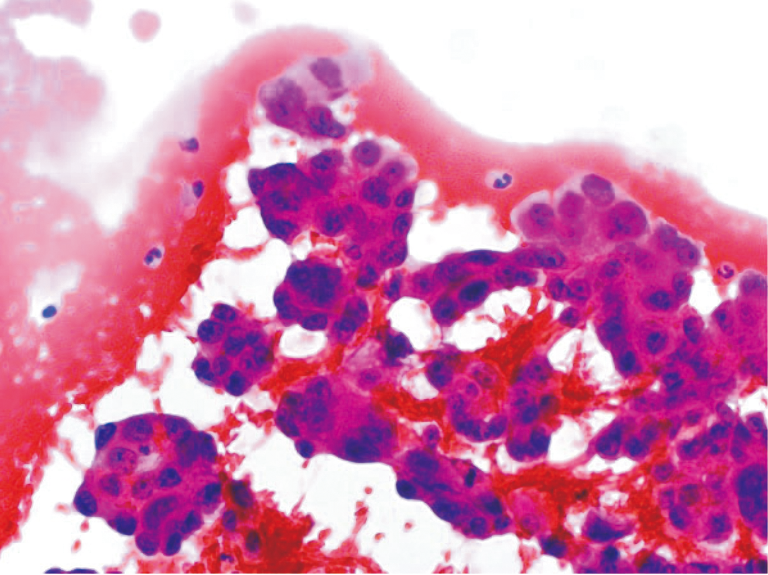
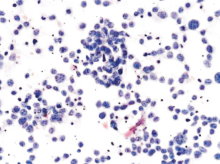
Figure 2
Case 2, thyroid metastatic small cell carcinoma of lung (FNA) The tumor cells were uniform in size, bare nucleus, with pepper salt like, fine granular chromatin, scattered or clustered (HE, ×400).
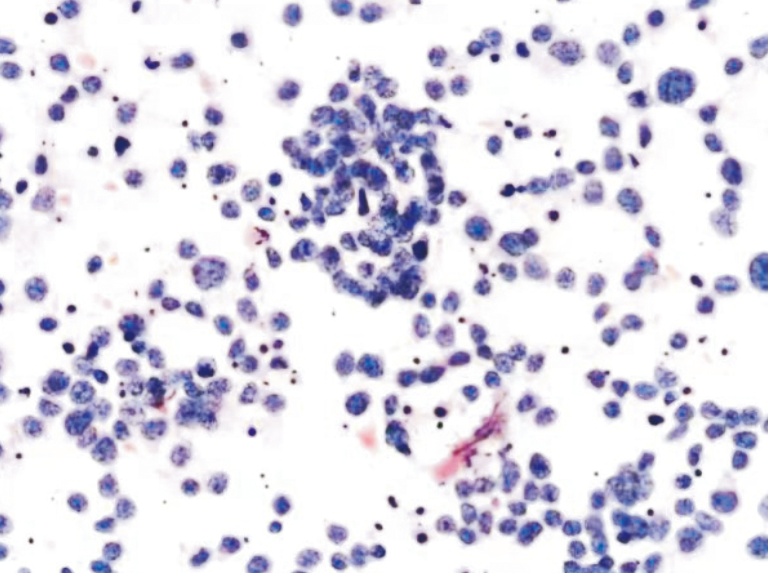
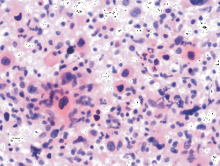
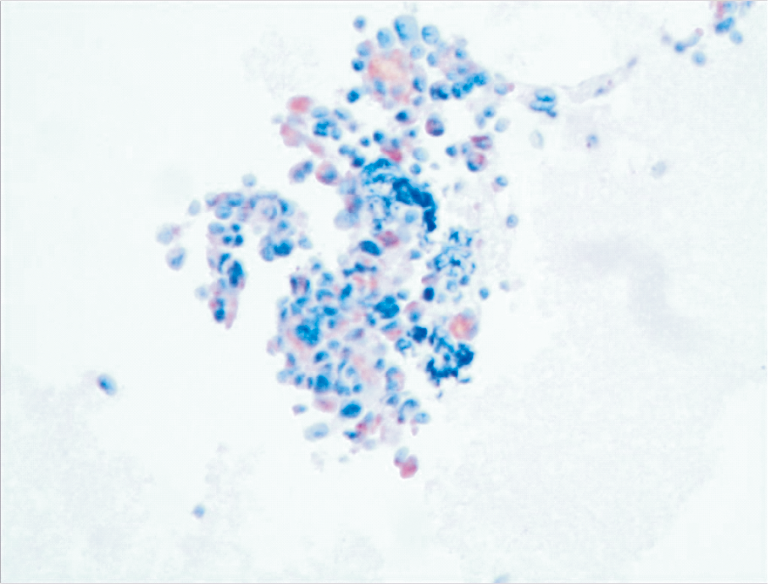
Figure 3
Case 8, Metastatic squamous cell carcinoma of thyroid The tumor cells were isolated, the nuclei varied in size, hyperchromatic, the cytoplasm was rich and eosinophilic, and cytoplasmic keratosis was observed (HE, ×400)
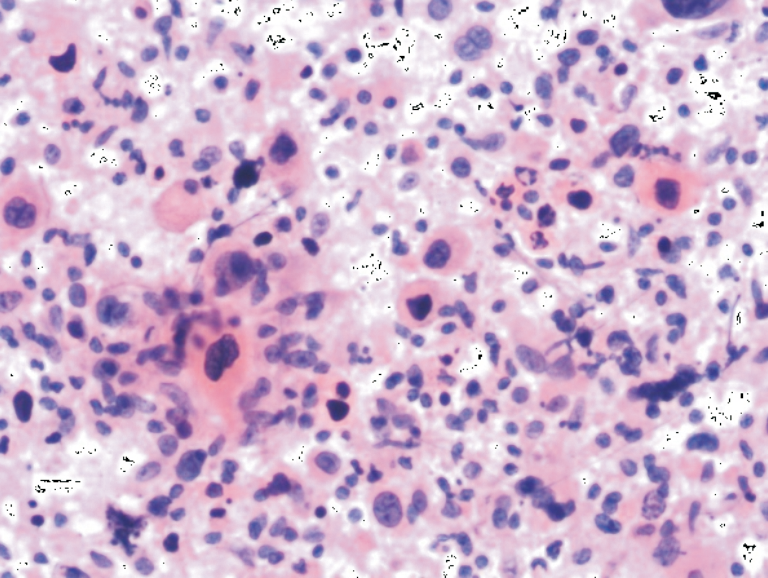
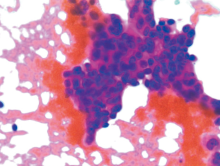
Figure 4
Case 4, Metastatic breast cancer of thyroid The tumor cells were distributed in sheets, the nuclei varied in size, hyperchromatic and irregular morphology (HE, ×400)
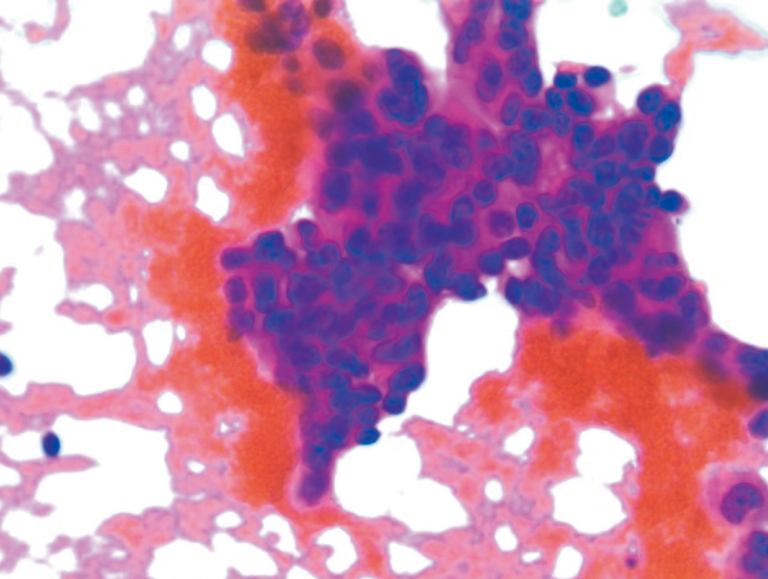
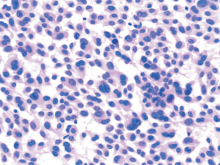
Figure 5
Medullary carcinoma (HE, ×400) Mainly scattered tumor cells, epithelioid, plasmacytoid, strange giant cells can be seen.
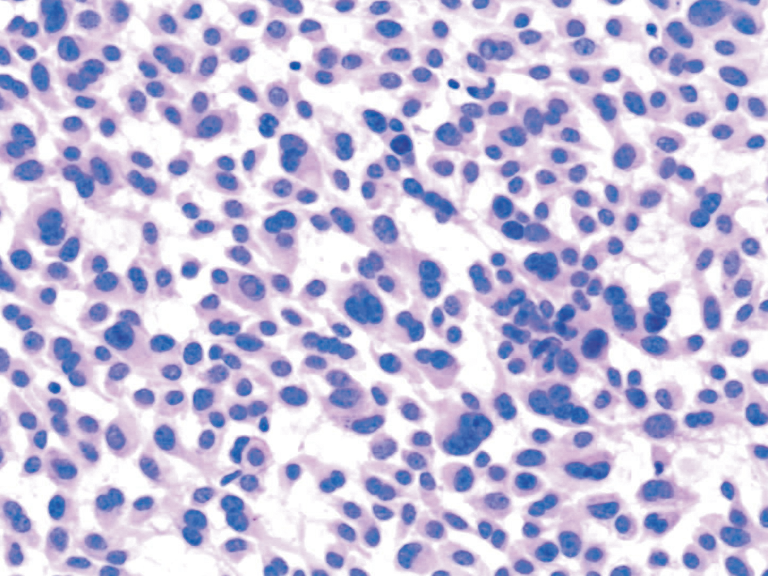
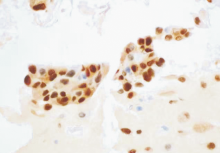
Figure 6
Breast cancer cells (Case 4) (IHC, ×400) ER is positive
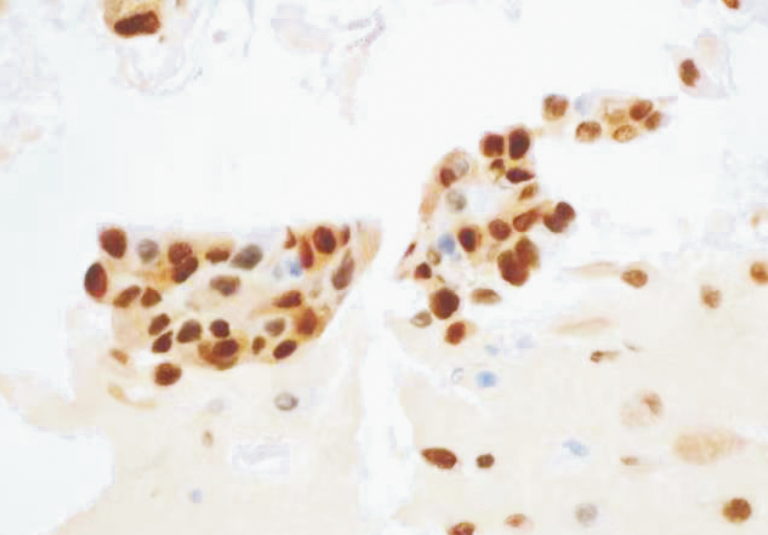
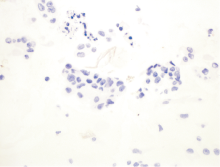
Figure 7
breast cancer cells (Case 4) (IHC, ×400) CT is negative
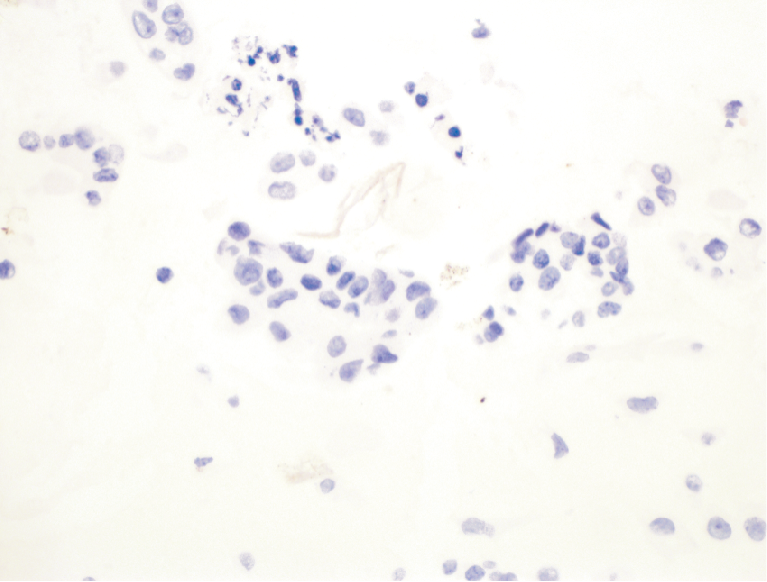
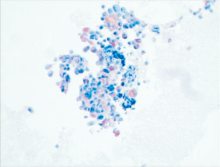
Figure 8
Medullary carcinoma (IHC, ×400) CT is positive
| [1] |
PUSZTASZERI M, WANG H, CIBAS E S, et al. Fine-needle aspiration biopsy of secondary neoplasms of the thyroid gland: a multi-institutional study of 62 cases[J]. Cancer Cytopathol, 2015, 123(1):19-29.
doi: 10.1002/cncy.21494 pmid: 25369542 |
| [2] |
MIRALLIÉ E, RIGAUD J, MATHONNET M, et al. Mana-gement and prognosis of metastases to the thyroid gland[J]. J Am Coll Surg, 2005, 200(2):203-207.
doi: 10.1016/j.jamcollsurg.2004.10.009 URL |
| [3] |
ZHANG L, LIU Y, LI X, et al. Metastases to the thyroid gland: A report of 32 cases in PUMCH[J]. Medicine (Baltimore), 2017, 96(36):e7927.
doi: 10.1097/MD.0000000000007927 URL |
| [4] |
BATTISTELLA E, POMBA L, MATTARA G, et al. Metastases to the thyroid gland: review of incidence, clinical presentation, diagnostic problems and surgery, our experience[J]. J Endocrinol Invest, 2020, 43(11):1555-1560.
doi: 10.1007/s40618-020-01282-w |
| [5] |
HOOKIM K, GAITOR J, LIN O, et al. Secondary tumors involving the thyroid gland: A multi-institutional analysis of 28 cases diagnosed on fine-needle aspiration[J]. Diagn Cytopathol, 2015, 43(11):904-911.
doi: 10.1002/dc.23331 pmid: 26302896 |
| [6] |
HEGEROVA L, GRIEBELER M L, REYNOLDS J P, et al. Metastasis to the thyroid gland: report of a large series from the Mayo Clinic[J]. Am J Clin Oncol, 2015, 38(4):338-342.
doi: 10.1097/COC.0b013e31829d1d09 URL |
| [7] |
KIM T Y, KIM W B, GONG G, et al. Metastasis to the thyroid diagnosed by fine-needle aspiration biopsy[J]. Clin Endocrinol (Oxf), 2005, 62(2):236-241.
doi: 10.1111/cen.2005.62.issue-2 URL |
| [8] |
BUŁA G, WALER J, NIEMIEC A, et al. Diagnosis of metastatic tumours to the thyroid gland by fine needle aspiration biopsy[J]. Endokrynol Pol, 2010, 61(5):427-429.
pmid: 21049452 |
| [9] |
PAPI G, FADDA G, CORSELLO S M, et al. Metastases to the thyroid gland: prevalence, clinicopathological aspects and prognosis: a 10-year experience[J]. Clin Endocrinol (Oxf), 2007, 66(4):565-571.
doi: 10.1111/cen.2007.66.issue-4 URL |
| [10] |
NIXON I J, COCA-PELAZ A, KALEVA A I, et al. Metastasis to the Thyroid Gland: A Critical Review[J]. Ann Surg Oncol, 2017, 24(6):1533-1539.
doi: 10.1245/s10434-016-5683-4 pmid: 27873099 |
| [11] |
MONTERO P H, IBRAHIMPASIC T, NIXON I J, et al. Thyroid metastasectomy[J]. J Surg Oncol, 2014, 109(1):36-41.
doi: 10.1002/jso.23452 pmid: 24122778 |
| [12] |
KO H M, JHU I K, YANG S H, et al. Clinicopathologic analysis of fine needle aspiration cytology of the thyroid. A review of 1,613 cases and correlation with histopathologic diagnoses[J]. Acta Cytol, 2003, 47(5):727-732.
doi: 10.1159/000326596 URL |
| [13] |
CIRIANO HERNÁNDEZ P, MARTÍNEZ PINEDO C, CALCERRADA ALISES E, et al. Colorectal cancer metastases to the thyroid gland: A case report[J]. World J Gastrointest Surg, 2020, 12(3):116-122.
doi: 10.4240/wjgs.v12.i3.116 pmid: 32218894 |
| [14] |
MANATAKIS D K, TASIS N, ANTONOPOULOU M I, et al. Colorectal cancer metastases to the thyroid gland-a systematic review : Colorectal cancer thyroid metastases[J]. Hormones (Athens), 2021, 20(1):85-91.
doi: 10.1007/s42000-020-00255-1 pmid: 33150571 |
| [15] |
WOOD K, VINI L, HARMER C. Metastases to the thyroid gland: the Royal Marsden experience[J]. Eur J Surg Oncol, 2004, 30(6):583-588.
doi: 10.1016/j.ejso.2004.03.012 URL |
| [16] |
CHUNG A Y, TRAN T B, BRUMUND K T, et al. Metastases to the thyroid: a review of the literature from the last decade[J]. Thyroid, 2012, 22(3):258-268.
doi: 10.1089/thy.2010.0154 pmid: 22313412 |
| [17] |
GHOSSEIN C A, KHIMRAJ A, DOGAN S, et al. Metastasis to the thyroid gland: a single-institution 16-year experience[J]. Histopathology, 2021, 78(4):508-519.
doi: 10.1111/his.v78.4 URL |
| [18] |
ROMERO ARENAS M A, RYU H, LEE S, et al. The role of thyroidectomy in metastatic disease to the thyroid gland[J]. Ann Surg Oncol, 2014, 21(2):434-439.
doi: 10.1245/s10434-013-3282-1 pmid: 24081800 |
| [1] | LI Xiaoshi, QIN Yue. Multiple radiology imaging techniques in the diagnosis of gout [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(03): 311-318. |
| [2] | WU Nanming, LI Jun, TAO Juan. Hot spots in diagnosis of malignant melanoma [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(03): 215-220. |
| [3] | HAO Jiaqi, WANG Xinlu, HU Xiaofan, PAN Xiaoxia, XU Jing, MA Jun. Clinical differential diagnosis of acute tubulointerstitial nephritis and acute tubular necrosis [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(02): 127-133. |
| [4] | XIE Yaqiong, LIN Xiaoyi. Value of serum-free light chain assay in differential diagnosis and staging of nephropathy of various etiologies [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(02): 166-171. |
| [5] | WANG Zhaohui, WU Haibo. Clinicopathological analysis of 31 cases of gastric schwannoma [J]. Journal of Diagnostics Concepts & Practice, 2021, 20(06): 552-556. |
| [6] | GUO Yan, GE Juanjuan, CHEN Chen, YIN Jiming, WANG Xiaolong, CHEN Jiageng, DU Yanwei, DUAN Yuanyuan, FAN Xuelin, ZHENG Lei, WANG Xiyong, ZHAN Weiwei, ZHANG Lu. Diagnostic value of fine needle aspiration biopsy combining with RJ-TIRADS in distinguishing benign and malignant thyroid nodules in elderly patients [J]. Journal of Diagnostics Concepts & Practice, 2020, 19(03): 286-291. |
| [7] | WANG Jianjun, CHEN Ya, FAN Xiangshan, NIU Fengnan. Sclerosing angiomatoid nodular transformation of spleen: clinicopathological analysis and literature review [J]. Journal of Diagnostics Concepts & Practice, 2019, 18(05): 560-564. |
| [8] | CHANG Rui, XU Jiaxu, DONG Haipeng, WU Mengxiong, ZHAO Xuesong, MIAO Fei, YAN Fuhua. Value of CT spectral imaging in the evaluation of Crohn's disease activity [J]. Journal of Diagnostics Concepts & Practice, 2019, 18(04): 432-435. |
| [9] | YANG Ruxue, LI Nan, ZHOU Ting, ZHAO Yan, CHEN Shaohua, ZHU Qing, FENG Zhenzhong. Clinicopathologic analysis of skin melanocyte lesions [J]. Journal of Diagnostics Concepts & Practice, 2018, 17(05): 566-571. |
| [10] | WU Xinyang, ZHANG Huan, PAN Zilai, TAN Jingwen, GAO Xiaoyuan. The diagnostic value of dual-source CT in differentiating primary gastric lymphoma from advanced gastric cancer [J]. Journal of Diagnostics Concepts & Practice, 2018, 17(01): 60-65. |
| [11] | LI Qinqin, YE Tingjun, MAO Minjing. A contrast analysis of thyroid ultrasound-guided fine needle aspiration cytology and thyroid ultrasound imaging reporting and data system [J]. Journal of Diagnostics Concepts & Practice, 2017, 16(06): 607-611. |
| [12] | ZHU Peipei, ZOU Jue, CHEN Jun, XU Rongrong, YAN Hongzhu. Intracranial solitary fibrous tumor/hemangiopericytoma: a clinicopathologic study of 20 cases with review of literature [J]. Journal of Diagnostics Concepts & Practice, 2017, 16(06): 622-626. |
| [13] | YI Lin, XIAO Li, CHEN Yan, YIN Yulei. Anaplastic large cell lymphoma: a clinicopathological study and review of literature [J]. Journal of Diagnostics Concepts & Practice, 2017, 16(03): 313-319. |
| [14] | . [J]. Journal of Diagnostics Concepts & Practice, 2014, 13(05): 491-494. |
| [15] | . [J]. Journal of Diagnostics Concepts & Practice, 2013, 12(02): 170-174. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||