Journal of Diagnostics Concepts & Practice ›› 2024, Vol. 23 ›› Issue (06): 612-618.doi: 10.16150/j.1671-2870.2024.06.008
Previous Articles Next Articles
LU Hongyu1, LIU Hong2, SONG Luxi2( )
)
Received:2024-04-05
Online:2024-12-25
Published:2024-12-25
Contact:
SONG Luxi
E-mail:songluxi@139.com
CLC Number:
LU Hongyu, LIU Hong, SONG Luxi. Analysis of clinical and laboratory characteristics of six cases with T-cell large granular lymphocytic leukemia[J]. Journal of Diagnostics Concepts & Practice, 2024, 23(06): 612-618.
Table 1
Clinical characteristics of T-LGLL
| No. | Gender (Male/Femal) | Age (Years) | Clinical symptoms | Time to diagnosis (month) | WBC (×109/L) | ANC (×109/L) | HGB (g/L) | Plt (×109/L) | LYM (%) | Absolute count of LGL(×109/L) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 59 | Anaemia,TD,splenomegaly | 87 | 2.5 | 0.4 | 49 | 15 | 80.8 | 0.4 |
| 2 | F | 57 | Anaemia, fever, lymphadenopathy | 13 | 3.6 | 1.4 | 63 | 46 | 52.2 | 1.0 |
| 3 | F | 68 | Anaemia,TD | 60 | 3.1 | 1.8 | 61 | 242 | 40.5 | 0.6 |
| 4 | F | 70 | Anaemia | 6 | 2.3 | 0.7 | 65 | 135 | 62.5 | 1.2 |
| 5 | M | 54 | anaemia,splenomegaly | 12 | 5.4 | 1.6 | 67 | 167 | 68.0 | 1.4 |
| 6 | M | 61 | Anaemia splenomegaly | 12 | 3.5 | 2.0 | 37 | 377 | 43.0 | 0.9 |
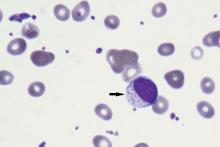
Figure 1
Morphology of T-cell large granular lymphocyte leukemia Peripheral blood smear demonstrating circulating atypical cell with an irregular nuclear contour, coarse chromatin, and azurophilic granules consistent with a large granular lymphocyte (arrow)(Wright’s stain,×100).

Table 2
Immunophenotype of T-LGLL patients
| No. | Proportion of T-LGL(%) | mCD3 | CD4 | CD8 | CD5 | CD7 | CD2 | TCRαβ | TCRγδ | CD57 | CD56 | CD16 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 9.6 | + | - | + | Dim | + | + | + | - | - | - | - |
| 2 | 13.6 | + | - | + | ND | P+ | + | + | - | P+ | - | - |
| 3 | 1.8 | + | - | + | Dim | + | + | + | - | - | - | - |
| 4 | 66.5 | + | - | + | - | Dim | + | + | - | + | - | - |
| 5 | 34.2 | + | - | + | Dim | Dim | + | + | - | + | - | + |
| 6 | 9.6 | + | + | + | + | + | + | + | - | + | - | - |
Table 3
Clonality rearrangement, genetic and molecular biological characteristics of T-LGLL cells
| No. | TCR rearrangement | Gene segments | Karyotypy | NGS mutation | Location | VAF(%) |
|---|---|---|---|---|---|---|
| 1 | TCRD+ TCRB+ | Vδ+Dδ+Jδ regions 152.01 bp Vβ+Jβ1/2 regions 265.45 bp | 46,XY[5] | STAT3 | Y640F | 24.5 |
| 2 | TCRB+ TCRG+ | Vβ+Jβ1/2 regions 167 bp Vγf-Jg1.3/2.3 regions 219 bp | 46,XX[8] | EP300 KMT2D | A922E P530A | 55 51.4 |
| 3 | TCRB+ TCRG+ | Vβ+Jβ1/2 regions 189 bp Vγ10-Jγ1.3/2.3 regions 219 bp | 46,XX[20] | STAT3 APC | Y640F T1496S | 3 49.1 |
| 4 | TCRD+ TCRB+ TCRG+ | Vδ+Dδ+Jδregions 212 bp Vβ+Jβ1/2 regions 184 bp Vγ10-Jγ1.3/2.3 regions 164 bp | 46,XX[1] | STAT3 KMT2D TP53 | S614R R2471* E271A | 28 5.8 50.9 |
| 5 | TCRB+ | Vβ+Jβ1/2 regions 179 bp | 46,XY[20] | TET2 | M1522I | 46.6 |
| 6 | TCRB+ TCRG+ | Vβ+Jβ1/2 regions 257 and 262 bp Vγ10-Jγ1.3/2.3 regions 148 bp Vγf-Jg1.3/2.3 regions 216 bp Vγf-Jg1.1/2.1 regions 237 bp | 46,XY[20] | STAT3 KMT2D ANKRD11 | Y640F Q2341Gfs Y808C | 7.9 3.8 47.1 |
| [1] | SHAH M V, HOOK C C, CALL T G, et al. A population-based study of large granular lymphocyte leukemia[J]. Blood Cancer J, 2016, 6(8):e455. |
| [2] |
ALAGGIO R, AMADOR C, ANAGNOSTOPOULOS I, et al. The 5th edition of the World Health Organization classification of haematolymphoid tumours: lymphoid neoplasms[J]. Leukemia, 2022, 36(7):1720-1748.
doi: 10.1038/s41375-022-01620-2 pmid: 35732829 |
| [3] | 中国中西医结合学会检验医学专业委员会. 流式细胞术临床检验图文报告书写专家共识[J]. 中华检验医学杂志, 2024, 47(7):729-739. |
| Chinese Society of Integrated Traditional Chinese and Western Medicine Laboratory Medicine Professional Committee. Expert consensus on writing graphic and textual reports for clinical testing of flow cytometry[J]. Chin J Lab Med, 2024, 47(7):729-739. | |
| [4] | JAFFE E S, ARBER D A, CAMPO E, et al. Hematopathology 2nd[J]. Elsevier, 2017,599-608. |
| [5] |
DONG N, CASTILLO TOKUMORI F, et al. Large granular lymphocytic leukemia - a retrospective study of 319 cases[J]. Am J Hematol, 2021, 96(7):772-780.
doi: 10.1002/ajh.26183 pmid: 33819354 |
| [6] | ZHU Y, GAO Q, HU J, et al. Clinical features and treatment outcomes in patients with T-cell large granular lymphocytic leukemia: a single-institution experience[J]. Leuk Res, 2020, 90:106299. |
| [7] |
MOHAN S R, MACIEJEWSKI J P. Diagnosis and therapy of neutropenia in large granular lymphocyte leukemia[J]. Curr Opin Hematol, 2009, 16(1):27-34.
doi: 10.1097/MOH.0b013e32831c8407 pmid: 19057202 |
| [8] | 石茵, 李元媛, 刘燕, 等. 髓系肿瘤合并克隆性T大颗粒淋巴细胞增殖的临床及实验室特征[J]. 中华血液学杂志, 2020, 41(4):276-281. |
| SHI Y, LI Y Y, LIU Y, et al. Clinical and laboratory characteristics of clonal T large granular lymphocyte proliferation in myeloid tumors[J]. Chin J Hematol, 2020, 41(4):276-281. | |
| [9] |
BAREAU B, REY J, HAMIDOU M, et al. Analysis of a French cohort of patients with large granular lymphocyte leukemia: a report on 229 cases[J]. Haematologica, 2010, 95(9):1534-1541.
doi: 10.3324/haematol.2009.018481 pmid: 20378561 |
| [10] |
CLEMENTE M J, WLODARSKI M W, MAKISHIMA H, et al. Clonal drift demonstrates unexpected dynamics of the T-cell repertoire in T-large granular lymphocyte leukemia[J]. Blood, 2011, 118(16):4384-4393.
doi: 10.1182/blood-2011-02-338517 pmid: 21865345 |
| [11] |
LAMY T, LOUGHRAN T P JR. How I treat LGL leukemia[J]. Blood, 2011, 117:2764-2774.
doi: 10.1182/blood-2010-07-296962 pmid: 21190991 |
| [12] | MELENHORST J J, SORBARA L, KIRBY M, et al. Large granular lymphocyte leukaemia is characterized by a clonal T-cell receptor rearrangement in both memory and effector CD8(+) lymphocyte populations[J]. Br J Haematol, 2001, 112(1):189-194. |
| [13] |
MOIGNET A, HASANALI Z, ZAMBELLO R, et al. Cyclophosphamide as a first-line therapy in LGL leukemia[J]. Leukemia, 2014, 28(5):1134-1136.
doi: 10.1038/leu.2013.359 pmid: 24280867 |
| [1] | AN Huihui, WU Tao, LIU Wenhui, TIAN Sirui. A Mendelian randomized study on the correlation between 91 inflammatory protein levels and the risk of acute myeloid leukemia [J]. Journal of Diagnostics Concepts & Practice, 2024, 23(5): 509-516. |
| [2] | ZHU Weiwei, LI Qian, WU Fan, ZHAI Zhimin. Gene mutations and their relationship with clinical features in 100 patients with myelodysplastic syndrome [J]. Journal of Diagnostics Concepts & Practice, 2024, 23(03): 305-312. |
| [3] | LIU Juan, YIN Lijuan, FAN Desheng. The clinicopathologic significance of AR, SKP2, SOX10, PD-L1 and TILs expression in triple-negative breast cancer [J]. Journal of Diagnostics Concepts & Practice, 2024, 23(02): 162-172. |
| [4] | YE Xiangjun, LU Xingguo. Interpretation of the 5th edition of the WHO classification of haematolymphoid tumours on MDS and AML [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(05): 421-428. |
| [5] | ZHANG Jiao, LÜ Jiajia, LU Wenli, ZHANG Lidan, LI Wei. Pediatric chronic myeloid leukemia with a BCR- FIBCD1-ABL1 fusion transcript: a case report and literature review [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(05): 472-479. |
| [6] | GAO Yanting, ZHAO Jinyan, WANG Juan, LI Jia, XU Wen, LI Li, LIN Lihui. Analysis of bone marrow lymphocyte subsets in patients with acute myeloid leukemia and its clinical significance [J]. Journal of Diagnostics Concepts & Practice, 2020, 19(04): 407-413. |
| [7] | PENG Zhenping, XIANG Xixi, ZHANG Sujiang, LI Jiaming. Chronic neutrophilic leukemia with leukemia-like reaction as the first-onset manifestation: a report of 2 cases and literature review [J]. Journal of Diagnostics Concepts & Practice, 2020, 19(02): 122-128. |
| [8] | LI Jiaming, ZHANG Sujiang, WANG Ying, YAN Zeying, LIU Zhiyin, SUN Haimin, CHEN Yubao, CHEN Yu, LUO Fangxiu, SUN Jing. Chronic myelomonocytic leukemia accompanied with extranodal lymphoma : a clinical feature analysis [J]. Journal of Diagnostics Concepts & Practice, 2018, 17(01): 76-81. |
| [9] | BAO Pingping, WU Chunxiao, ZHANG Minlu, GU Kai, XIANG Yongmei, PENG Peng, GONG Yangming, SHI Liang, ZOU Zhen.. Epidemiological features of major subtypes of leukemia and its incidence trends in Shanghai [J]. Journal of Diagnostics Concepts & Practice, 2017, 16(05): 484-491. |
| [10] | WANG Shu, ZHANG Yunxiang, SUI Jingni, LU Jing, FAN Huiyong, WANG Chao, CHEN Bing.. Analysis of additional mutation pattern accompanied with CEBPA mutations in patients with the cytogenetically normal acute myeloid leukemia [J]. Journal of Diagnostics Concepts & Practice, 2017, 16(05): 498-503. |
| [11] | ZHU Jianyi, LANG Wenjing, CHEN Fangyuan, XU Zhuoran, SHEN Lijing, ZHONG Jihua. Effect of arsenic trioxide on EVI1 gene in regulating hematopoietic transcription factors in vitro [J]. Journal of Diagnostics Concepts & Practice, 2017, 16(01): 42-47. |
| [12] | . [J]. Journal of Diagnostics Concepts & Practice, 2016, 15(01): 25-29. |
| [13] | . [J]. Journal of Diagnostics Concepts & Practice, 2015, 14(04): 363-366. |
| [14] | . [J]. Journal of Diagnostics Concepts & Practice, 2015, 14(04): 329-333. |
| [15] | . [J]. Journal of Diagnostics Concepts & Practice, 2015, 14(03): 235-238. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||