Journal of Diagnostics Concepts & Practice ›› 2023, Vol. 22 ›› Issue (02): 127-133.doi: 10.16150/j.1671-2870.2023.02.004
• Original article • Previous Articles Next Articles
HAO Jiaqi1,2, WANG Xinlu1, HU Xiaofan1, PAN Xiaoxia1, XU Jing1( ), MA Jun1()
), MA Jun1()
Received:2023-02-16
Online:2023-04-25
Published:2023-08-31
CLC Number:
HAO Jiaqi, WANG Xinlu, HU Xiaofan, PAN Xiaoxia, XU Jing, MA Jun. Clinical differential diagnosis of acute tubulointerstitial nephritis and acute tubular necrosis[J]. Journal of Diagnostics Concepts & Practice, 2023, 22(02): 127-133.
Figure 1
Proportion of ATIN in renal biopsy and AKD
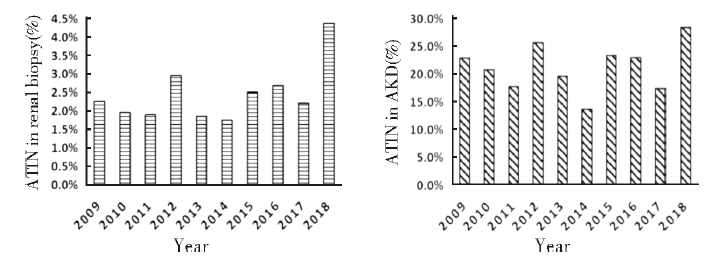
Table 1
The comparison of clinical characteristics between ATN and ATIN
| Indice | ATN(n=109) | ATIN(n=135) | P |
|---|---|---|---|
| Male(%) | 72(66.1%) | 58(43.0%) | <0.01 |
| Age(year) | 49(15-85) | 53(14-82) | 0.09 |
| BMI(kg/m2) | 24.6±3.9 | 22.9±3.6 | <0.01 |
| AKD disease course(%) | 82(75.2%) | 60(44.4%) | <0.01 |
| AKI(%) | 70(64.2%) | 20(14.8%) | <0.01 |
| Urgent dialysis needed during hospitalization (%) | 43(39.4%) | 26(19.3%) | <0.01 |
| Dialysis independent at hospital discharge(%) | 22(51.2%) | 20(76.9%) | 0.03 |
| Clinical manifestation | |||
| Fever(%) | 23(21.1%) | 40(29.6%) | 0.12 |
| Rash(%) | 9(8.3%) | 10(7.4%) | 0.08 |
| Arthralgia(%) | 6(5.5%) | 4(3.0%) | 0.32 |
| Oliguria(%) | 53(48.6%) | 23(17.0%) | <0.01 |
| Inducement | |||
| Infection(%) | 22(20.2%) | 31(23.0%) | 0.60 |
| Toxicant(%) | 8(7.3%) | 2(1.5%) | 0.05 |
| Drugs(%) | 30(27.5%) | 34(25.2%) | 0.68 |
| Unknown(%) | 49(45.0%) | 68(50.4%) | 0.40 |
| Hypertension(%) | 39(35.8%) | 52(38.5%) | 0.66 |
| Diabetes(%) | 8(7.3%) | 11(8.1%) | 0.82 |
Table 2
The comparison of laboratory findings between ATN and ATIN
| Indice | ATN(n=109) | ATIN(n=135) | P |
|---|---|---|---|
| Scr at admission(μmol/L) | 314(81-2 290) | 238(101-876) | <0.01 |
| Peak Scr (μmol/L) | 425(102-2 290) | 278(115-1 270) | <0.01 |
| Scr at discharge(μmol/L) | 264(54-1 059) | 171.5(50-876) | 0.66 |
| Prealbumin(mg/L) | 225.1±78.7 | 225.1±61.6 | 1.00 |
| Alb(g/L) | 26(8-46) | 34(12-43) | <0.01 |
| Uric acid(μmol/L) | 454(149-874) | 345(104-779) | <0.01 |
| TG(mmol/L) | 2.1(0.8-15.1) | 1.7(0.5-7.0) | <0.01 |
| TC(mmol/L) | 5.1(0.9-21.8) | 4.4(1.6-19.8) | <0.01 |
| PTH(pg/mL)* | 1.9±0.4 | 1.9±0.4 | 0.30 |
| Hb(g/L) | 116.7±29.8 | 100.9±20.9 | <0.01 |
| BCR | 14.6±11.0 | 11.8±5.4 | 0.02 |
| 24 h urine protein(mg/24 h) | 1 350(52-23 555) | 1 036(75-27 303) | 0.31 |
| hematuria(%) | 0.54 | ||
| Gross hematuria(%) | 11(10.1%) | 12(8.9%) | |
| Microscopic hematuria(%) | 41(37.6%) | 43(31.9%) | |
| Urinary sodium/Potassium ratio | 2.2(0.1-15.8) | 2.8(0.2-21.5) | 0.04 |
| Urinary urea nitrogen (mmol/24 h)# | 12.9±4.2 | 12.6±4.4 | 0.57 |
Table 3
Logistic regression analysis of factors in ATIN
| Indice | Single factor regression | Multiple regression | |||
|---|---|---|---|---|---|
| OR(95%CI) | P | OR(95%CI) | P | ||
| Clinical data | |||||
| Female(%) | 2.58(1.53-4.36) | <0.01 | - | - | |
| Age(year) | 1.01(1.00-1.03) | 0.07 | - | - | |
| Non-AKI | 10.3(5.58-19.1) | <0.01 | - | - | |
| Non-oliguria | 4.61(2.57-8.27) | <0.01 | - | - | |
| BMI | 0.88(0.82-0.96) | <0.01 | - | - | |
| Treatment | |||||
| Urgent dialysis unneeded during hospitalization | 2.73(1.54-4.85) | <0.01 | - | - | |
| Dialysis independent at hospital discharge | 3.18(1.07-9.47) | 0.04 | - | - | |
| Laboratory examination | |||||
| Scr at admission(μmol/L) | 0.998(0.997-0.999) | <0.01 | 0.997(0.995-0.999) | <0.01 | |
| Alb(g/L) | 1.06(1.03-1.09) | <0.01 | 1.05(1.01-1.09) | 0.01 | |
| UA(μmol/L) | 0.995(0.993-0.997) | <0.01 | 0.997(0.994-0.999) | 0.01 | |
| TG(mmol/L) | 0.68(0.53-0.86) | <0.01 | - | ||
| TC(mmol/L) | 0.82(0.73-0.91) | <0.01 | - | ||
| Hb(g/L) | 0.98(0.97-0.99) | <0.01 | 0.97(0.95-0.98) | <0.01 | |
| Urinary sodium/Potassium ratio | 1.02(0.93-1.12) | 0.65 | - | ||
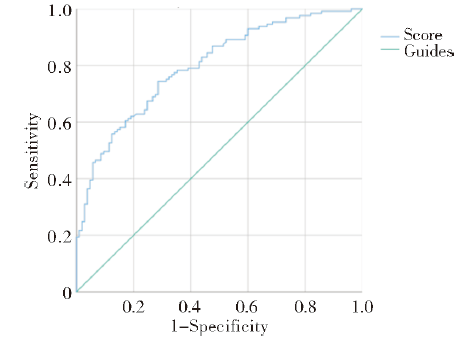
Figure 2
ROC curve for the differential diagnosis of ATIN and ATN by four indicators combined model
| [1] |
ULINSKI T, SELLIER-LECLERC A L, TUDORACHE E, et al. Acute tubulointerstitial nephritis[J]. Pediatr Nephrol, 2012, 27(7):1051-1057.
doi: 10.1007/s00467-011-1915-9 pmid: 21638156 |
| [2] |
JOYCE E, GLASNER P, RANGANATHAN S, et al. Tubulointerstitial nephritis: diagnosis, treatment, and monitoring[J]. Pediatr Nephrol, 2017, 32(4):577-587.
doi: 10.1007/s00467-016-3394-5 pmid: 27155873 |
| [3] | GEDIK G K, YILMAZ F, KAYA B, et al. Mercaptoacetyltriglycine renal scan for the differential diagnosis of acute tubular necrosis and interstitial nephritis associated to vancomycin[J]. Rev Esp Med Nucl Imagen Mol, 2012, 31(3):155-157. |
| [4] |
JOAQUIM A I, MENDES G E, RIBEIRO P F, et al. Ga-67 scintigraphy in the differential diagnosis between acute interstitial nephritis and acute tubular necrosis: an experimental study[J]. Nephrol Dial Transplant, 2010, 25(10):3277-3282.
doi: 10.1093/ndt/gfq152 URL |
| [5] | SCHWARTZ M M. Tubulointerstitial diseases and infections of the kidney[M]// JENNETTE J C, OLSON J L, SCHWARTZ M M, et al. 5th ed. Philadelphia: Lippincott Williams & Wilkins, 2015:657-890. |
| [6] |
PRAGA M, SEVILLANO A, AUÑÓN P, et al. Changes in the aetiology, clinical presentation and management of acute interstitial nephritis, an increasingly common cause of acute kidney injury[J]. Nephrol Dial Transplant, 2015, 30(9):1472-1479.
doi: 10.1093/ndt/gfu326 URL |
| [7] |
GOICOECHEA M, RIVERA F, LÓPEZ-GÓMEZ J M, et al. Increased prevalence of acute tubulointerstitial nephritis[J]. Nephrol Dial Transplant, 2013, 28(1):112-115.
doi: 10.1093/ndt/gfs143 URL |
| [8] |
BOMBACK A S, MARKOWITZ G S. Increased prevalence of acute interstitial nephritis: more disease or simply more detection?[J]. Nephrol Dial Transplant, 2013, 28(1):16-18.
doi: 10.1093/ndt/gfs318 URL |
| [9] |
KIM H, JO S K, AHN S Y, et al. Long-term renal outcome of biopsy-proven acute tubular necrosis and acute interstitial nephritis[J]. J Korean Med Sci, 2020, 35(26):e206.
doi: 10.3346/jkms.2020.35.e206 URL |
| [10] |
RUEBNER R L, FADROWSKI J J. Tubulointerstitial nephritis[J]. Pediatr Clin North Am, 2019, 66(1):111-119.
doi: 10.1016/j.pcl.2018.08.009 URL |
| [11] |
CHAWLA L S, BELLOMO R, BIHORAC A, et al. Acute kidney disease and renal recovery: consensus report of the Acute Disease Quality Initiative (ADQI) 16 Workgroup[J]. Nat Rev Nephrol, 2017, 13(4):241-257.
doi: 10.1038/nrneph.2017.2 pmid: 28239173 |
| [12] |
SU T, GU Y, SUN P, et al. Etiology and renal outcomes of acute tubulointerstitial nephritis: a single-center prospective cohort study in China[J]. Nephrol Dial Transplant, 2018, 33(7):1180-1188.
doi: 10.1093/ndt/gfx247 URL |
| [13] |
BAKER R J, PUSEY C D. The changing profile of acute tubulointerstitial nephritis[J]. Nephrol Dial Transplant, 2004, 19(1):8-11.
doi: 10.1093/ndt/gfg464 URL |
| [14] |
BUYSEN J G, HOUTHOFF H J, KREDIET R T, et al. Acute interstitial nephritis: a clinical and morphological study in 27 patients[J]. Nephrol Dial Transplant, 1990, 5(2):94-99.
doi: 10.1093/ndt/5.2.94 URL |
| [15] |
SCHWARZ A, KRAUSE P H, KUNZENDORF U, et al. The outcome of acute interstitial nephritis: risk factors for the transition from acute to chronic interstitial nephritis[J]. Clin Nephrol, 2000, 54(3):179-190.
pmid: 11020015 |
| [16] | 马杰, 文煜冰, 吴海婷, 等. 55例急性间质性肾炎的临床特点及病因分析[J]. 临床药物治疗杂志, 2021, 19(5):51-55. |
| MA J, WEN Y B, WU H T, et al. Clinical characteristics and etiological study of 55 patients with acute interstitial nephritis[J]. Clin Med J, 2021, 19(5):51-55. | |
| [17] | 刘小庆, 王墨. 199例儿童急性间质性肾炎临床及预后分析[J]. 重庆医科大学学报, 2020, 45(11):1573-1578. |
| LIU X Q, WANG M. Clinical and prognostic analysis of 199 children with acute interstitial nephritis[J]. J Chong-qing Med Univ, 2020, 45(11):1573-1578. | |
| [18] |
HOWELL M, SEBIRE N J, MARKS S D, et al. Biopsy-proven paediatric tubulointerstitial nephritis[J]. Pediatr Nephrol, 2016, 31(10):1625-1630.
doi: 10.1007/s00467-016-3374-9 pmid: 27139900 |
| [19] | 任海滨, 俞香宝, 孙彬, 等. 53例急性间质性肾炎临床病理分析[J]. 临床肾脏病杂志, 2013, 13(11):519-522. |
| REN H B, YU X B, SUN B, et al. Clinicopathological analysis of 53 cases of acute interstitial nephritis[J]. J Clin Nephrol, 2013, 13(11):519-522. | |
| [20] | 张燕京, 李晓玫. 药物相关肾实质性急性肾衰竭患者的贫血特征、红细胞生成素水平及其与肾损害的关系[J]. 北京大学学报(医学版), 2005, 37(5):471-475. |
| ZHANG Y J, LI X M. Relationship among the characteristics of anemia, serum level of erythropoietin and the renal tubulointerstitial injury in drug-associated renal parenchymal acute renal failure patients[J]. J Peking Univ (Health Sci) 2005, 37(5):471-475. | |
| [21] |
LEE T, YANG W S. Non-diabetic glycosuria as a diagnostic clue for acute tubulointerstitial nephritis in patients with azotemia[J]. Ren Fail, 2020, 42(1):1015-1021.
doi: 10.1080/0886022X.2020.1824923 pmid: 32985319 |
| [22] |
SALVADOR L G, CAROLINA G F, JESÚS R D, et al. A low BUN/creatinine ratio predicts histologically confirmed acute interstitial nephritis[J]. BMC Nephrol, 2023, 24(1):75.
doi: 10.1186/s12882-023-03118-0 pmid: 36967386 |
| [23] |
PERAZELLA M A, MARKOWITZ G S. Drug-induced acute interstitial nephritis[J]. Nat Rev Nephrol, 2010, 6(8):461-470.
doi: 10.1038/nrneph.2010.71 pmid: 20517290 |
| [24] |
URBSCHAT A, OBERMÜLLER N, HAFERKAMP A. Biomarkers of kidney injury[J]. Biomarkers, 2011, 16(Suppl 1):S22-S30.
doi: 10.3109/1354750X.2011.587129 URL |
| [25] |
MOLEDINA D G, WILSON F P, POBER J S, et al. Urine TNF-α and IL-9 for clinical diagnosis of acute interstitial nephritis[J]. JCI Insight, 2019, 4(10):e127456.
doi: 10.1172/jci.insight.127456 URL |
| [1] | XIE Yaqiong, LIN Xiaoyi. Value of serum-free light chain assay in differential diagnosis and staging of nephropathy of various etiologies [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(02): 166-171. |
| [2] | LIN Xia, GAO Chao, HUANG Pei, WANG Gang, LIN Guozhen, REN Rujing. Analysis of clinical and imaging manifestations in 8 patients with MOGAG and literature review [J]. Journal of Diagnostics Concepts & Practice, 2022, 21(05): 606-612. |
| [3] | WANG Zhaohui, WU Haibo. Clinicopathological analysis of 31 cases of gastric schwannoma [J]. Journal of Diagnostics Concepts & Practice, 2021, 20(06): 552-556. |
| [4] | HU Ying, BAO Yujie, BAI Yupan, LU Guanzhu, CHENG Yajiao, GUO Zhuying, XU Jie. Analysis of clinical and laboratory characteristics of EB virus infection in 67 adult patients [J]. Journal of Diagnostics Concepts & Practice, 2020, 19(1): 74-79. |
| [5] | SHI Dongmei, WANG Xiaolin, CHEN Lu, XIE Qing. Clinical characteristics and misdiagnosis analysis of sparganosis:A retrospective study of 52 cases [J]. Journal of Diagnostics Concepts & Practice, 2020, 19(1): 37-43. |
| [6] | YANG Qiao, WEN Yuting, YANG Changwei. Five cases of the malignant melanoma with serosal effusion: the clinical and pathological analysis [J]. Journal of Diagnostics Concepts & Practice, 2020, 19(05): 499-503. |
| [7] | WANG Juan, WANG Kaiwen, ZHAO Jiangfeng. Value of anti-melanoma differentiation-related gene 5 antibody for assessing disease activity and prognosis in patients with dermatomyositis-associated interstitial lung disease [J]. Journal of Diagnostics Concepts & Practice, 2019, 18(2): 155-159. |
| [8] | WANG Jianjun, CHEN Ya, FAN Xiangshan, NIU Fengnan. Sclerosing angiomatoid nodular transformation of spleen: clinicopathological analysis and literature review [J]. Journal of Diagnostics Concepts & Practice, 2019, 18(05): 560-564. |
| [9] | CHANG Rui, XU Jiaxu, DONG Haipeng, WU Mengxiong, ZHAO Xuesong, MIAO Fei, YAN Fuhua. Value of CT spectral imaging in the evaluation of Crohn's disease activity [J]. Journal of Diagnostics Concepts & Practice, 2019, 18(04): 432-435. |
| [10] | YANG Ruxue, LI Nan, ZHOU Ting, ZHAO Yan, CHEN Shaohua, ZHU Qing, FENG Zhenzhong. Clinicopathologic analysis of skin melanocyte lesions [J]. Journal of Diagnostics Concepts & Practice, 2018, 17(05): 566-571. |
| [11] | WU Xinyang, ZHANG Huan, PAN Zilai, TAN Jingwen, GAO Xiaoyuan. The diagnostic value of dual-source CT in differentiating primary gastric lymphoma from advanced gastric cancer [J]. Journal of Diagnostics Concepts & Practice, 2018, 17(01): 60-65. |
| [12] | ZHU Peipei, ZOU Jue, CHEN Jun, XU Rongrong, YAN Hongzhu. Intracranial solitary fibrous tumor/hemangiopericytoma: a clinicopathologic study of 20 cases with review of literature [J]. Journal of Diagnostics Concepts & Practice, 2017, 16(06): 622-626. |
| [13] | LU Xiaoxue, DA Qian. Clinical characteristics and pathological features of Kimura disease: report of 13 case and review of literature [J]. Journal of Diagnostics Concepts & Practice, 2017, 16(06): 639-644. |
| [14] | YI Lin, XIAO Li, CHEN Yan, YIN Yulei. Anaplastic large cell lymphoma: a clinicopathological study and review of literature [J]. Journal of Diagnostics Concepts & Practice, 2017, 16(03): 313-319. |
| [15] | . [J]. Journal of Diagnostics Concepts & Practice, 2014, 13(05): 491-494. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||