诊断学理论与实践 ›› 2024, Vol. 23 ›› Issue (01): 46-56.doi: 10.16150/j.1671-2870.2024.01.007
丁景峰1, 敖炜群2, 朱珍1, 孙静1, 徐良根1, 郑世保1, 俞晶晶1, 胡金文1( )
)
收稿日期:2023-10-30
出版日期:2024-02-25
发布日期:2024-05-30
通讯作者:
胡金文 E-mail: hufeng678678@163.com基金资助:
DING Jingfeng1, AO Weiqun2, ZHU Zhen1, SUN Jing1, XU Lianggen1, ZHENG Shibao1, YU Jingjing1, HU Jinwen1()
Received:2023-10-30
Published:2024-02-25
Online:2024-05-30
摘要:
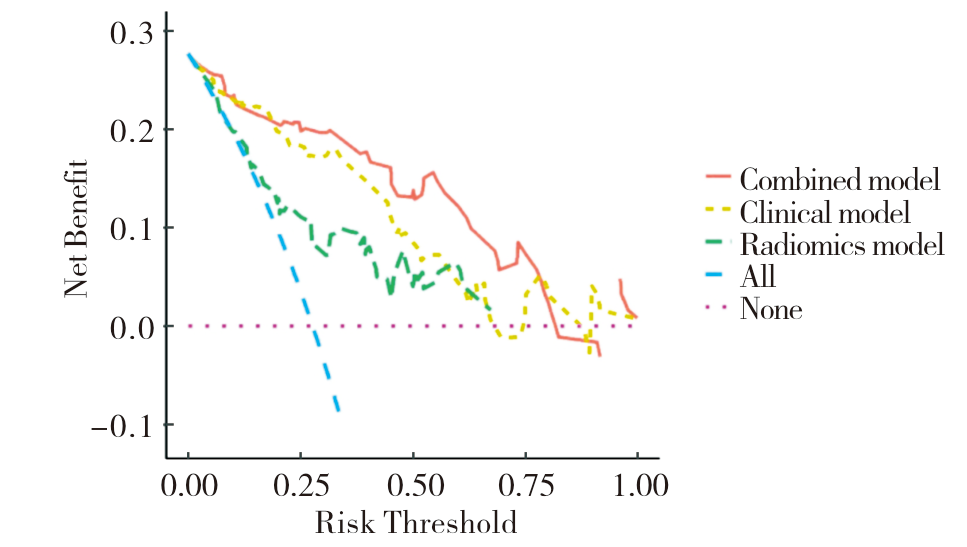
目的: 探讨基于磁共振(magnetic resonance imaging,MRI)T2加权成像(T2-weighted imaging,T2WI)和弥散加权成像(diffusion-weighted imaging,DWI)的影像组学,在术前预测直肠癌壁外血管侵犯(extramural vascular invasion, EMVI)的诊断效能。方法: 回顾性收集2010年1月至2023年6月经术后病理证实为直肠腺癌且术前行直肠MRI扫描的患者168例,按7∶3随机分为训练集和验证集。提取T2WI、DWI的影像组学特征,采用最大相关最小冗余 (the maximum relevance minimum redundancy,mRMR)和十倍交叉验证的最小绝对收缩与选择算子(the least absolute shrinkage and selection operator,LASSO)回归分析降维并选择影像组学特征,计算每例患者的影像组学总评分(Radscore),使用Radscore建立影像组学模型。在训练集中,研究纳入了3个临床特征[年龄、性别、术前癌胚抗原(carcinoembryonic antigen,CEA)]和6个磁共振影像学特征[ADC值、浸润深度、肿瘤长度、肿瘤部位、T分期、MRI壁外血管侵犯(magnetic resonance imaging-defined EMVI, mrEMVI)评分],通过单因素、多因素Logistic回归分析建立临床模型。联合Radscore和临床模型的独立危险因素,建立临床-影像组学模型(联合模型)。采用受试者操作特征(receiver operating characteristic, ROC)曲线评估各模型的诊断效能,通过DeLong检验比较不同模型的效能差异,采用校准曲线评估列线图术前预测结果与术后病理真实状况的拟合度,运用决策曲线分析(decision curve analysis, DCA)评价3种模型的临床应用价值。结果: 联合模型、临床模型、影像组学模型ROC曲线在训练集和验证集中AUC分别为0.926、0.888、0.756和0.917、0.896、0.782,联合模型的诊断效能最佳。Delong检验显示,在训练集和验证集中,联合模型诊断效能高于影像组学模型(P<0.05);在训练集中,联合模型的诊断效能高于临床模型(P<0.05),但在验证集中差异无统计学意义(P>0.05)。校准曲线显示列线图术前预测结果与术后病理结果一致性良好(P<0.05)。DCA结果表明,当风险阈值概率在0.24~0.77时,联合模型在临床上的获益高于临床模型和影像组学模型。结论: 基于T2WI和DWI的MRI影像组学模型术前预测直肠癌EMVI有较高的诊断效能,联合临床模型中独立危险因素构建的临床-影像组学MRI模型(联合模型)进一步提高了诊断效能。
中图分类号:
丁景峰, 敖炜群, 朱珍, 孙静, 徐良根, 郑世保, 俞晶晶, 胡金文. 基于T2WI和DWI的磁共振影像组学在术前预测直肠癌壁外血管侵犯的价值研究[J]. 诊断学理论与实践, 2024, 23(01): 46-56.
DING Jingfeng, AO Weiqun, ZHU Zhen, SUN Jing, XU Lianggen, ZHENG Shibao, YU Jingjing, HU Jinwen. The value of radiomics based on T2WI and DWI of MRI in preoperative prediction of extramural vascular invasion in rectal cancer[J]. Journal of Diagnostics Concepts & Practice, 2024, 23(01): 46-56.
表1
MRI扫描参数
| Equipment | Parameters Plane | T2WI | DWI Axial | ||
|---|---|---|---|---|---|
| Axial oblique | Sagittal | Coronal | |||
| Siemens Verio 3.0T | TR/TE,ms | 4 000/97 | 4 000/97 | 4 000/97 | 9 700/93 |
| FOV,mm | 240×240 | 220×220 | 220×220 | 280×350 | |
| Thickness,mm | 3 | 3 | 3 | 3 | |
| b values | - | - | - | 0,800,1 500 | |
| Siemens Avanto 1.5T | TR/TE,ms | 4 120/97 | 3 940/85 | 4 990/96 | 4 912/95 |
| FOV,mm | 200×200 | 250×250 | 240×240 | 250×250 | |
| Thickness,mm | 2.5 | 4 | 4 | 5 | |
| b values | - | - | - | 50,400,800 | |
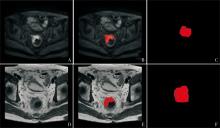
图1
病灶分割 A、D:分别为包含病灶的DWI、T2WI原始图像;B、E:分别为DWI及T2WI上分割病灶后的图像,红色区域代表图像上分割的肿瘤区域;C,F:分别为DWI及T2WI上生成的三维掩模;红色区域代表逐层分割肿瘤后,ITK-SNAP软件自动生成的三维掩模。
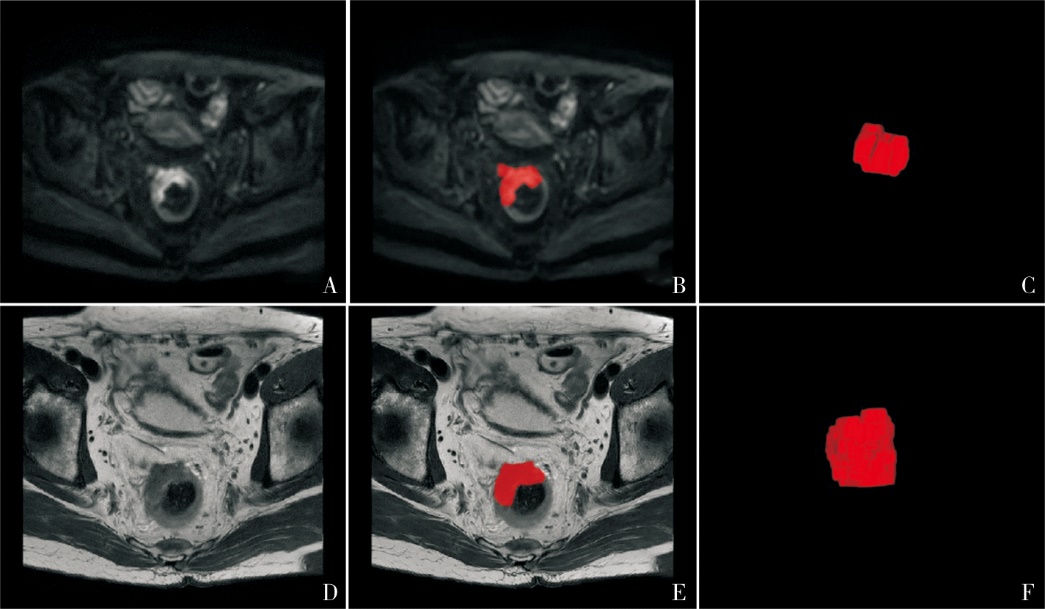
表2
训练集与验证集患者的临床、影像学、病理学特征
| Characteristics | Training set (n=123) | Validation set (n=45) | t/χ2 | P value |
|---|---|---|---|---|
| Age(years) | 63.82±10.38 | 64.47±10.96 | 0.352 | 0.726 |
| Gender(%) | 0.164 | 0.686 | ||
| Male | 78(63.4) | 27(60.0) | ||
| Female | 45(36.6) | 18(40.0) | ||
| CEA(%) | 0.323 | 0.570 | ||
| ≤5 ng/mL | 77(62.6) | 26(57.8) | ||
| >5 ng/mL | 46(37.4) | 19(42.2) | ||
| ADC Value (×10-3mm2/s) | 0.81(0.72,0.91) | 0.78(0.71,0.87) | -1.091 | 0.275 |
| Infiltration depth (mm) | 15.34±5.73 | 16.61±8.09 | 1.130 | 0.260 |
| Length,(cm) | 43.14±15.78 | 44.50±15.56 | 0.496 | 0.621 |
| mrT stage(%) | 0.235 | 0.628 | ||
| T1~2 | 46(37.4) | 15(33.3) | ||
| T3~4 | 77(62.6) | 30(66.7) | ||
| mrEMVI(%) | 0.362 | 0.547 | ||
| Negative | 80(65.0) | 27(60.0) | ||
| Positive | 43(35.0) | 18(40.0) | ||
| pEMVI(%) | 0.016 | 0.900 | ||
| Negative | 89(72.4) | 33(73.3) | ||
| Positive | 34(27.6) | 12(26.7) | ||
| Radscore | -2.71(-3.87,-1.32) | -2.09(-3.87,-1.20) | -1.067 | 0.286 |
表3
训练集和验证集中病理EMVI阳性与阴性组间的临床、影像学特征比较
| Characteristics | Training set | Validation set | |||||
|---|---|---|---|---|---|---|---|
| EMVI(-)(n=89) | EMVI(+)(n=34) | P value | EMVI(-)(n=33) | EMVI(+)(n=12) | P value | ||
| Age(years) | 64.31±10.42 | 62.53±10.30 | 0.396 | 63.7±12.1 | 66.7±6.9 | 0.423 | |
| Gender(%) | 0.814 | 0.063 | |||||
| Male | 32(36.0) | 13(38.2) | 10(30.3) | 8(66.7) | |||
| Female | 57(64.0) | 21(61.8) | 23(69.7) | 4(33.3) | |||
| CEA (%) | 0.171 | 0.097 | |||||
| ≤5 ng/mL | 59(66.3) | 18(52.9) | 22(66.7) | 4(33.3) | |||
| >5 ng/mL | 30(33.7) | 16(47.1) | 11(33.3) | 8(66.7) | |||
| ADC Value(×10-3mm2/s) | 0.85(0.74,0.99) | 0.75(0.61,0.80) | <0.001 | 0.82(0.72,0.93) | 0.75(0.68,0.79) | 0.066 | |
| Infiltration Depth(mm) | 14.63±6.03 | 17.20±4.39 | 0.011 | 14.9±5.1 | 21.4±12.3 | 0.101 | |
| Length,(cm) | 41.18±15.51 | 48.27±15.54 | 0.025 | 43.3±14.2 | 47.9±19.0 | 0.387 | |
| Location (%) | 0.683 | 0.060# | |||||
| Upper | 27(30.3) | 8(23.5) | 11(33.3) | 0(0.0) | |||
| Middle | 35(39.3) | 16(47.1) | 12(36.4) | 6(50.0) | |||
| Low | 27(30.3) | 10(29.4) | 10(30.3) | 6(50.0) | |||
| mrT stage(%) | <0.001 | 0.074 | |||||
| T1-2 | 42(47.2) | 4(11.8) | 14(42.4) | 1(8.3) | |||
| T3-4 | 47(52.8) | 30(88.2) | 19(57.6) | 11(91.7) | |||
| mrEMVI(%) | <0.001 | <0.001 | |||||
| Negative | 71(79.8) | 9(26.5) | 26(78.8) | 1 (8.3) | |||
| Positive | 18(20.2) | 25(73.5) | 7 (21.2) | 11(91.7) | |||
| Radscore | -3.14(-4.44,-2.08) | -1.40(-2.69,-0.69) | <0.001 | -2.46(-4.19,-1.39) | -1.25(-1.74,-0.18) | 0.004 | |
图2
LASSO 10折交叉验证图 A: (T2WI)用10倍交叉验证的方法寻找 LASSO的超参数lambda,垂直虚线为最佳lambda值;B:(DWI)图像中每条彩色的线代表特征的系数随 lambda 值的变化曲线,垂直虚线为最佳lambda取值时获得的非零特征。
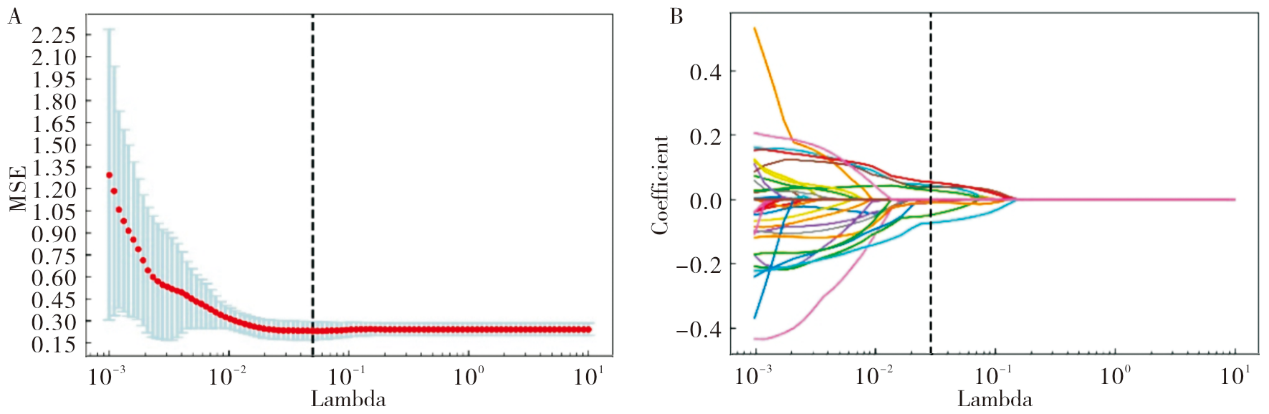
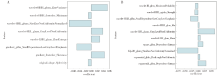
图3
筛选的最佳特征及其权重系数 A: 基于DWI筛选出的8个最佳特征;B: 基于T2WI筛选出的10个最佳特征。
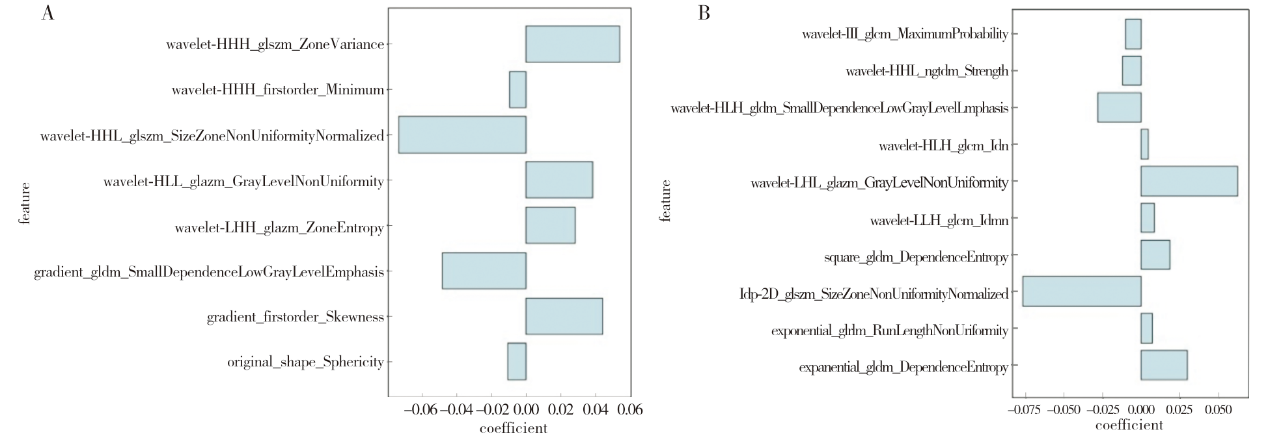
表4
单变量和多变量逻辑回归分析结果
| Variables | Univariate | Multivariate(clinical model) | Multivariate(combined model) | |||||
|---|---|---|---|---|---|---|---|---|
| OR(95% CI) | P value | OR(95% CI) | P value | OR(95% CI) | P value | |||
| Age | 0.983(0.946~1.022) | 0.393 | ||||||
| Gender | ||||||||
| Female | ||||||||
| Male | 0.907(0.401~2.051) | 0.814 | ||||||
| CEA | ||||||||
| ≤5 ng/mL | ||||||||
| >5 ng/mL | 1.748(0.782~3.907) | 0.173 | ||||||
| ADC | 0.000(0.000~0.012) | <0.001 | 0.000(0.000~0.016) | <0.001 | 0.000(0.000~0.016) | 0.001 | ||
| Infiltration depth | 1.085(1.008~1.167) | 0.029 | ||||||
| Length | 1.030(1.003~1.058)) | 0.029 | ||||||
| Location | ||||||||
| upper | ||||||||
| middle | 1.543(0.576~4.136) | 0.389 | ||||||
| low | 1.250(0.428~3.651) | 0.683 | ||||||
| mrT stage | ||||||||
| T1~T2 | ||||||||
| T3~T4 | 6.702(2.180~20.607) | 0.001 | 2.869(0.778~10.574) | 0.113 | 3.899(0.940~16.172) | 0.061 | ||
| mrEMVI | ||||||||
| Negative | ||||||||
| Positive | 10.957(4.363~27.518) | <0.001 | 8.643(2.886~25.886) | <0.001 | 7.928(2.397~26.221) | 0.001 | ||
| Radscore | 1.862(1.336~2.596) | <0.001 | 2.048(1.301~3.226) | 0.002 | ||||

图4
影像组学模型、临床模型和联合模型的ROC曲线
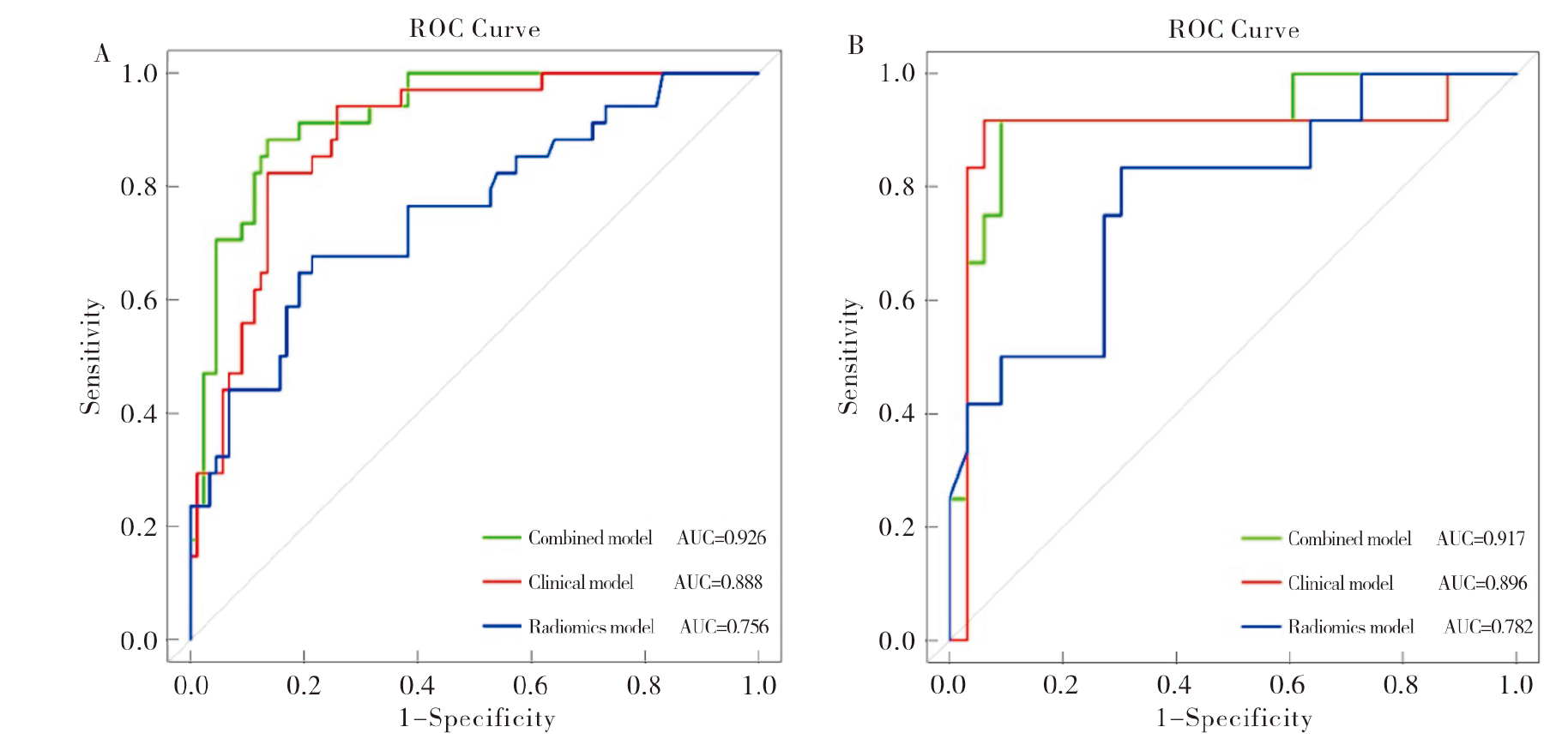
表5
训练集与验证集中不同模型的预测效能
| Models | Training set | Validation set | |||||
|---|---|---|---|---|---|---|---|
| AUC(95% CI) | Sensitivity | Specificity | AUC(95% CI) | Sensitivity | Specificity | ||
| Radiomics model | 0.756(0.656~0.855) | 0.676 | 0.787 | 0.782(0.626~0.937) | 0.833 | 0.697 | |
| Clinical model | 0.888(0.829~0.948) | 0.824 | 0.865 | 0.896(0.753~1.000) | 0.917 | 0.939 | |
| Combined model | 0.926(0.879~0.973) | 0.882 | 0.865 | 0.917(0.813~1.000) | 0.917 | 0.909 | |
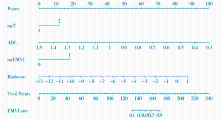
图5
基于联合模型可视化列线图
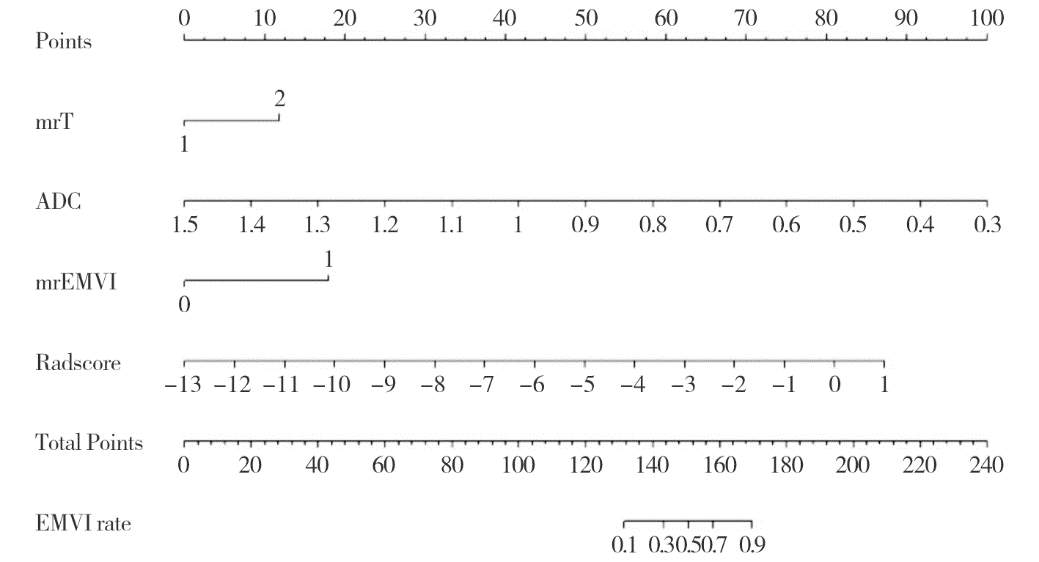
图6
列线图校正曲线
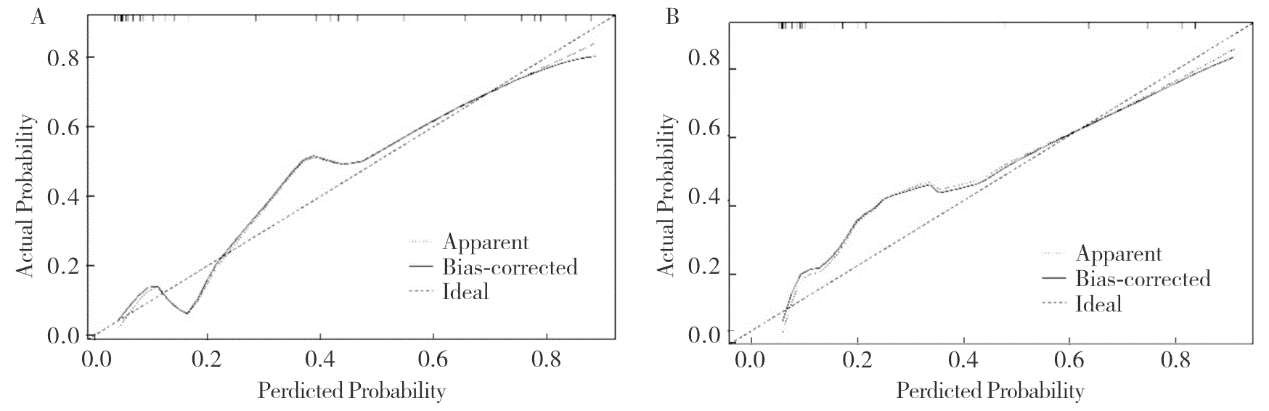
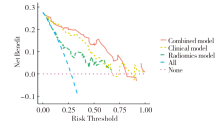
图7
列线图的决策分析曲线
| [1] | XIA C, DONG X, LI H, et al. Cancer statistics in China and United States, 2022: profiles, trends, and determinants[J]. Chin Med J (Engl), 2022, 135(5):584-590. |
| [2] |
VAN DEN BROEK J J, VAN DER WOLF F S W, HEIJNEN L A, et al. The prognostic importance of MRI detected extramural vascular invasion (mrEMVI) in locally advanced rectal cancer[J]. Int J Colorectal Dis, 2020, 35(10):1849-1854.
doi: 10.1007/s00384-020-03632-9 pmid: 32488420 |
| [3] | SCHAAP D P, VOOGT E L K, BURGER J W A, et al. Prognostic implications of mri-detected emvi and tumor deposits and their response to neoadjuvant therapy in cT3 and cT4 rectal cancer[J]. Int J Radiat Oncol Biol Phys, 2021, 111(3):816-825. |
| [4] | TAN J J, CARTEN R V, BABIKER A, et al. Prognostic importance of MRI-detected extramural venous invasion in rectal cancer: a literature review and systematic meta-analysis[J]. Int J Radiat Oncol Biol Phys, 2021, 111(2):385-394. |
| [5] | 杨鋆, 辛城霖, 张忠涛. 中低位直肠癌的精准诊断与规范治疗[J]. 中华消化外科杂志, 2024, 23(1):85-90. |
| YANG Y, XIN C L, ZHANG Z T. Precision diagnosis and standardized treatment of mid-low rectal cancer[J]. Chin J Dig Surg, 2024, 23(1):85-90. | |
| [6] | 中华医学会外科学分会腹腔镜与内镜外科学组, 中华医学会外科学分会结直肠外科学组, 中国医师协会外科医师分会结直肠外科专家工作组, 等. 腹腔镜结直肠癌根治术操作指南(2023版)[J]. 中华消化外科杂志, 2024, 23(1):10-22. |
| Laparoscopic & Endoscopic Surgery Group, Branch of Surgery, Chinese Medical Association; Colorectal Surgery Group, Branch of Surgery, Chinese Medical Association; Chinese Society of Colon and Rectal Surgeons, Chinese Medical Doctor Association, et al. Guideline for ope-rative procedure of laparoscopic radical surgery for colorectal cancer (2023 edition)[J]. Chin J Dig Surg, 2024, 23(1):10-22. | |
| [7] | 肖体先, 侯文运, 梅世文, 等. 早发性结直肠癌的临床病理特征[J]. 中华消化外科杂志, 2023, 22(12):1476-1483. |
| XIAO T X, HOU W Y, MEI S W, et al. Clinical characteristics of early-onset colorectal cancer[J]. Chin J Dig Surg, 2023, 22(12):1476-1483. | |
| [8] | 应俊, 孙亚煌, 王安琪, 等. 基于SEER数据库直肠癌肝转移预后列线图预测模型的构建及其应用价值[J]. 中华消化外科杂志, 2023, 22(S1):51-57. |
| YING J, SUN Y H, WANG A Q, et al. Construction and application value of nomogram predictive model for the prognosis of rectal cancer liver metastases based on SEER database[J]. Chin J Dig Surg, 2023, 22(S1):51-57. | |
| [9] |
SMITH N J, BARBACHANO Y, NORMAN A R, et al. Prognostic significance of magnetic resonance imaging-detected extramural vascular invasion in rectal cancer[J]. Br J Surg, 2008, 95(2):229-236.
doi: 10.1002/bjs.5917 pmid: 17932879 |
| [10] |
BAE J S, KIM S H, HUR B Y, et al. Prognostic value of MRI in assessing extramural venous invasion in rectal cancer: multi-readers' diagnostic performance[J]. Eur Radiol, 2019, 29(8):4379-4388.
doi: 10.1007/s00330-018-5926-9 pmid: 30617483 |
| [11] | BROWN G, RADCLIFFE A G, NEWCOMBE R G, et al. Preoperative assessment of prognostic factors in rectal cancer using high-resolution magnetic resonance imaging[J]. Br J Surg, 2003, 90(3):355-364. |
| [12] | LAMBIN P, LEIJENAAR R T H, DEIST T M, et al. Radiomics: the bridge between medical imaging and persona-lized medicine[J]. Nat Rev Clin Oncol, 2017, 14(12):749-762. |
| [13] | YU X, SONG W, GUO D, et al. Preoperative prediction of extramural venous invasion in rectal cancer: comparison of the diagnostic efficacy of radiomics models and quantitative dynamic contrast-enhanced magnetic resonance imaging[J]. Front Oncol, 2020,10:459. |
| [14] | LIU S, YU X, YANG S, et al. Machine learning-based radiomics nomogram for detecting extramural venous invasion in rectal cancer[J]. Front Oncol, 2021,11:610338. |
| [15] | SHU Z, MAO D, SONG Q, et al. Multiparameter MRI-based radiomics for preoperative prediction of extramural venous invasion in rectal cancer[J]. Eur Radiol, 2022, 32(2):1002-1013. |
| [16] | KANDA T, MATSUDA M, OBA H, et al. Gadolinium deposition after contrast-enhanced MR imaging[J]. Radio-logy, 2015, 277(3):924-925. |
| [17] |
DUAN C, KALLEHAUGE J F, BRETTHORST G L, et al. Are complex DCE-MRI models supported by clinical data?[J]. Magn Reson Med, 2017, 77(3):1329-1339.
doi: 10.1002/mrm.26189 pmid: 26946317 |
| [18] | 国家卫生健康委员会医政司, 中华医学会肿瘤学分会. 国家卫健委中国结直肠癌诊疗规范(2023版)[J]. 中国实用外科杂志, 2023, 43(6):602-630. |
| Hospital Authority of National Health Commission ofthe People's Republic of China; Chinese Society ofOncology, Chinese Medical Association. Chinese protocol of diagnosis and treatment of colorectal cancer of the National Health Commission(2023 edition)[J]. Chin J Pract Surg, 2023, 43(6):602-630. | |
| [19] |
TALBOT I C, RITCHIE S, LEIGHTON M, et al. Invasion of veins by carcinoma of rectum: method of detection, histological features and significance[J]. Histopathology, 1981, 5(2):141-163.
doi: 10.1111/j.1365-2559.1981.tb01774.x pmid: 7216178 |
| [20] | BATES D D B, HOMSI M E, CHANG K J, et al. MRI for rectal cancer: staging, mrCRM, EMVI, lymph node staging and post-treatment response[J]. Clin Colorectal Cancer, 2022, 21(1):10-18. |
| [21] | GLYNNE-JONES R, WYRWICZ L, TIRET E, et al. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up[J]. Ann Oncol, 2017, 28(suppl_4):iv22-iv40. |
| [22] |
ZHAO L, LIANG M, WANG S, et al. Preoperative evaluation of extramural venous invasion in rectal cancer using radiomics analysis of relaxation maps from synthetic MRI[J]. Abdom Radiol (NY). 2021 Aug; 46(8):3815-3825.
doi: 10.1007/s00261-021-03021-y pmid: 33743017 |
| [23] | WANG H, CHEN X, DING J, et al. Novel multiparametric MRI-based radiomics in preoperative prediction of perirectal fat invasion in rectal cancer[J]. Abdom Radiol (NY), 2023, 48(2):471-485. |
| [24] | ROY S, MAJI P. Multispectral co-occurrence of wavelet coefficients for malignancy assessment of brain tumors[J]. PLoS One, 2021, 16(6):e0250964. |
| [25] | PENG Y, LUO Y, HU X, et al. Quantitative T2*-weighted imaging and reduced field-of-view diffusion-weighted imaging of rectal cancer: correlation of R2* and apparent diffusion coefficient with histopathological prognostic factors[J]. Front Oncol, 2021,11:670156. |
| [26] |
AO W, ZHANG X, YAO X, et al. Preoperative prediction of extramural venous invasion in rectal cancer by dynamic contrast-enhanced and diffusion weighted MRI: a preliminary study[J]. BMC Med Imaging, 2022, 22(1):78.
doi: 10.1186/s12880-022-00810-9 pmid: 35484509 |
| [27] | 吴德生, 梁烨鑫, 陈秀婵, 等. 高分辨T2WI在直肠癌壁外血管侵犯诊断中的应用价值[J]. 中国中西医结合影像学杂志, 2020, 18(6):548-551. |
| WU D S, LIANG Y X, CHEN X C, et al. Application value of high-resolution MRI T2WI in extramural vascular invasion of rectal cancer[J]. Chin Imag J Integr Tradit West Med, 2020, 18(6):548-551. | |
| [28] | 张益飞, 李月玥, 杨彦松, 等. 基于高分辨率T2WI的影像组学列线图预测直肠癌脉管侵袭的研究[J]. 中国临床医学影像杂志, 2021, 32(7):500-505. |
| ZHANG Y F, LI Y Y, YANG Y S, et al. High resolution T2WI-based radiomics nomogram for prediction of lymphovascular invasion in rectal cancer[J]. J China Clin Med Imag, 2021, 32(7):500-505. | |
| [29] | 王可欣, 余静, 徐青. 基于RESOLVE ADC的影像组学列线图在预测直肠癌壁外血管侵犯中的应用价值[J]. 肿瘤影像学, 2023, 32(2):138-147. |
| WANG K X, YU J, XU Q. Radiomics based on RESOLVE ADC in identification of extramural venous invasion in rectal cancer[J]. Oncoradiol, 2023, 32(2):138-147. |
| [1] | 李明, 陈克敏, 潘自来, 罗禹. CT及MRI预测急性缺血性脑梗死出血性转化的价值研究进展[J]. 诊断学理论与实践, 2024, 23(01): 83-89. |
| [2] | 钱丹烨, 孟祥军, 朱黎明. 京都胃炎评分及其改良预测模型在胃镜下判断中国人群幽门螺杆菌感染状态的价值[J]. 诊断学理论与实践, 2023, 22(06): 555-561. |
| [3] | 周熠磊, 张淼, 郭睿, 周金鑫, 李彪, 李翔. 18F-PSMA PET/MRI在早期诊断前列腺癌根治术后复发、转移中的价值[J]. 诊断学理论与实践, 2023, 22(06): 567-572. |
| [4] | 冯丽, 任刚, 蔡嵘, 汪心韵, 王辉, 祝明洁. 泌尿生殖系统血管周上皮样细胞瘤(PEComa)的临床特征分析[J]. 诊断学理论与实践, 2023, 22(05): 460-465. |
| [5] | 秦晓丹, 孙慧玲, 潘蓓, 潘玉琴, 王书奎. miR-1229-3p抑制结直肠癌疾病进展及作为潜在生物标志物的研究[J]. 诊断学理论与实践, 2023, 22(05): 429-440. |
| [6] | 李笑石, 秦越. 影像学技术在痛风诊断及疾病监测中的应用研究进展[J]. 诊断学理论与实践, 2023, 22(03): 311-318. |
| [7] | 陈乾, 林慧敏, 严福华. 磁共振成像评估肝功能储备的研究进展[J]. 诊断学理论与实践, 2023, 22(02): 190-196. |
| [8] | 李卫侠, 徐学勤, 朱晓雷, 陈克敏. 39例肾上腺皮质癌患者的CT、MRI影像特点及其诊断价值[J]. 诊断学理论与实践, 2023, 22(02): 134-140. |
| [9] | 李佳曦, 汪锦江, 俞立萍, 袁英, 乔光磊, 马俐君. RAB25沉默抑制结直肠癌细胞铁死亡的作用研究[J]. 诊断学理论与实践, 2022, 21(06): 710-718. |
| [10] | 杨蕊馨, 杜宇童, 燕然林, 朱正纲, 李琛, 于颖彦. 消化道肿瘤单细胞转录组测序研究中生物样本前处理改良的探索[J]. 诊断学理论与实践, 2022, 21(05): 567-574. |
| [11] | 杜燕然, 焦景, 任芸芸, 周建桥. 超声影像组学技术在评估胎肺成熟度中的应用[J]. 诊断学理论与实践, 2022, 21(03): 326-330. |
| [12] | 黄娟, 朱晓雷, 李晓, 陈克敏, 严福华, 徐学勤. 血氧水平依赖磁共振成像评估早期慢性肾病肾缺氧的研究[J]. 诊断学理论与实践, 2022, 21(03): 385-389. |
| [13] | 张华, 陆炜, 杨承翌, 项明洁. 血清人衰老关键蛋白1检测对结肠直肠癌的诊断和预后价值[J]. 诊断学理论与实践, 2021, 20(05): 462-465. |
| [14] | 朱乃懿, 姜奕歆, 柴丽, 柴维敏. 磁共振对超声阴性而乳腺X线检出BI-RADS4类以上钙化灶的诊断价值分析[J]. 诊断学理论与实践, 2021, 20(05): 439-444. |
| [15] | 张雪坤, 李彦, 严福华, 赵洪飞, 宋琦. 基于光梭成像的新型加速技术在颅脑MRI中的应用价值研究[J]. 诊断学理论与实践, 2021, 20(04): 378-383. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||