Journal of Diagnostics Concepts & Practice ›› 2025, Vol. 24 ›› Issue (05): 555-561.doi: 10.16150/j.1671-2870.2025.05.012
• Case reports • Previous Articles Next Articles
ZHENG Xiangyu1,2, CHEN Jinxiang1, LIU Guorong1, YANG Yaoxiang1, CAI Shaoting1, YANG Jing1( )
)
Received:2024-12-26
Revised:2025-07-08
Accepted:2025-08-22
Online:2025-10-25
Published:2025-10-23
Contact:
YANG Jing
E-mail:eyjingyang@scut.edu.cn
CLC Number:
ZHENG Xiangyu, CHEN Jinxiang, LIU Guorong, YANG Yaoxiang, CAI Shaoting, YANG Jing. Clinicopathological analysis and literature review of SMARCB1-deficient sinonasal carcinoma[J]. Journal of Diagnostics Concepts & Practice, 2025, 24(05): 555-561.
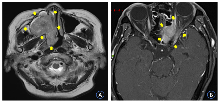
Figure 1
Head MRI image


Figure 2
Pathological images of case 1
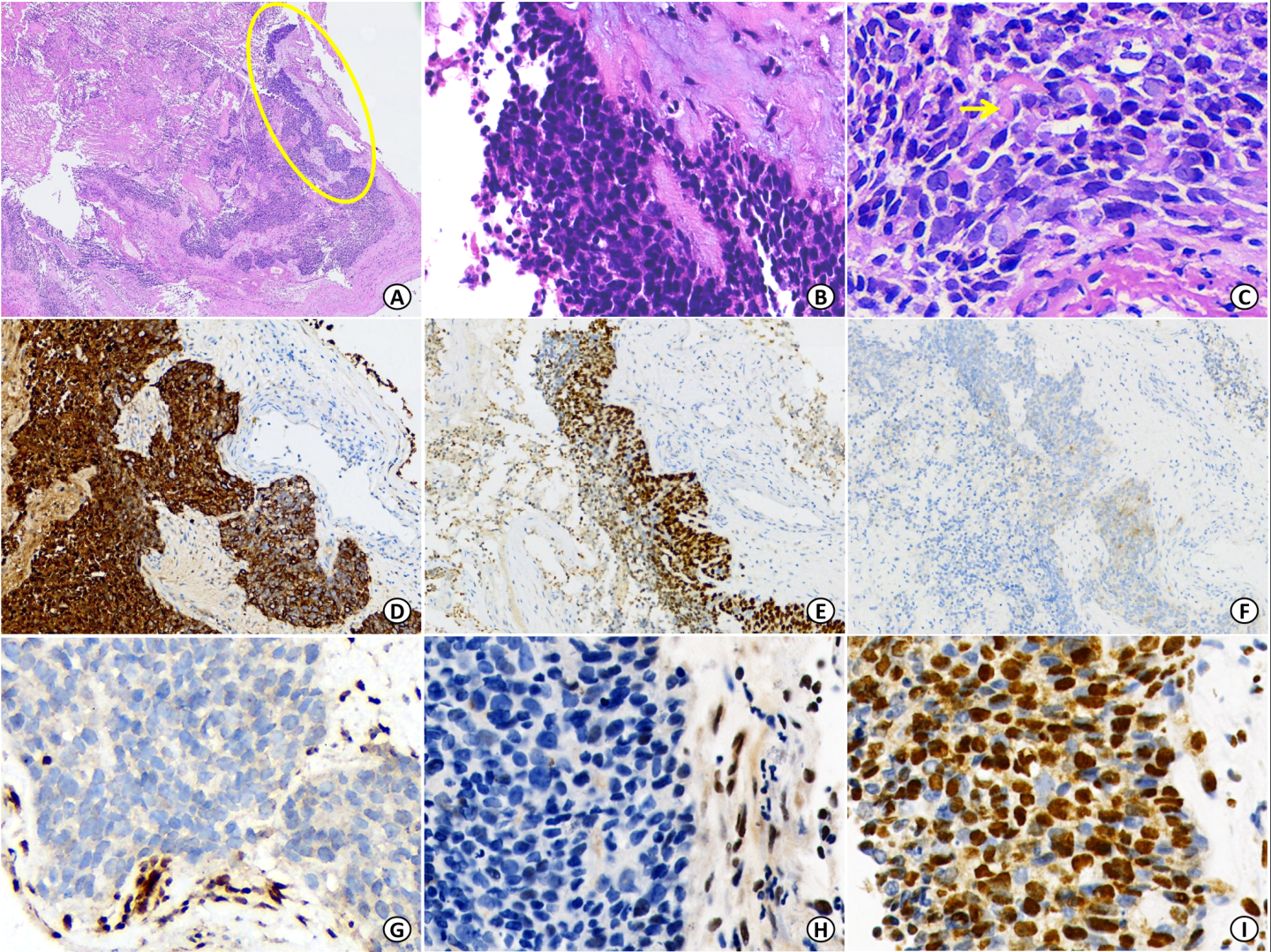

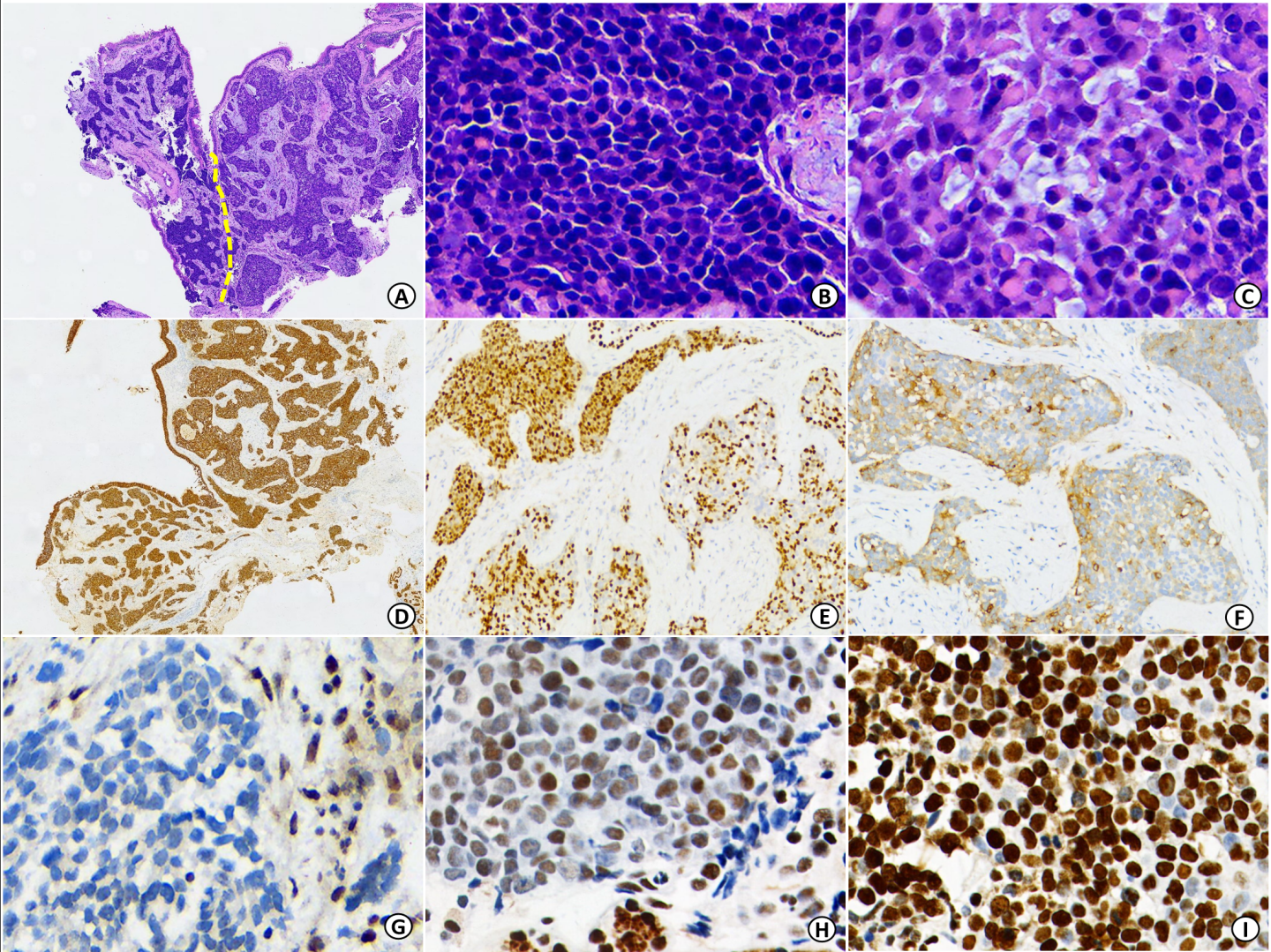
Figure 3
Pathological images of case 2
| [1] | AGAIMY A, DIN N U, JAIN D, et al. SWI/SNF complex-deficient sinonasal carcinoma[M/OL]. WHO classification of tumours editorial board. Head and neck tumours. Lyon (France): International Agency for Research on Cancer. 5th ed. 2023[2024-11-01]. https://tumourclassification.iarc.who.int/chapters/52. |
| [2] |
BISHOP J A, ANTONESCU C R, WESTRA W H. SMARCB1 (INI-1)-deficient carcinomas of the sinonasal tract[J]. Am J Surg Pathol, 2014, 38(9):1282-1289.
doi: 10.1097/PAS.0000000000000285 pmid: 25007146 |
| [3] |
AGAIMY A, KOCH M, LELL M, et al. SMARCB1(INI1)-deficient sinonasal basaloid carcinoma: a novel member of the expanding family of SMARCB1-deficient neoplasms[J]. Am J Surg Pathol, 2014, 38(9):1274-1281.
doi: 10.1097/PAS.0000000000000236 pmid: 24832165 |
| [4] | 汤申隽, 翟长文, 袁存存, 等. SMARCB1(INI1)缺失的鼻腔鼻窦癌六例临床病理学特征[J]. 中华病理学杂志, 2020, 49(1):47-51. |
| TANG S J, ZHAI C W, YUAN C C, et al. SMARCB1 (INI1)-deficient sinonasal carcinoma: a clinicopathological analysis of six cases[J]. Chin J Pathol, 2020, 49(1):47-51. | |
| [5] | LEE V H, TSANG R K, LO A W I, et al. SMARCB1 (INI-1)-deficient sinonasal carcinoma: A systematic review and pooled analysis of treatment outcomes[J]. Cancers (Basel), 2022, 14(13): 3285. |
| [6] |
AGAIMY A, HARTMANN A, ANTONESCU C R, et al. SMARCB1 (INI-1)-deficient sinonasal carcinoma: A series of 39 cases expanding the morphologic and clinicopathologic spectrum of a recently described entity[J]. Am J Surg Pathol, 2017, 41(4):458-471.
doi: 10.1097/PAS.0000000000000797 pmid: 28291122 |
| [7] | SKÁLOVÁ A, TAHERI T, BRADOVÁ M, et al. SMARCB1-deficient sinonasal adenocarcinoma: a rare variant of SWI/SNF-deficient malignancy often misclassified as high-grade non-intestinal-type sinonasal adenocarcinoma or myoepithelial carcinoma[J]. Virchows Arch, 2024, 485(2):245-256. |
| [8] |
NG J K M, CHAN J Y K, LI J J X, et al. SMARCB1 (INI1)-deficient sinonasal carcinoma with yolk sac differentiation showing Co-loss of SMARCA4 immunostaining - a case report and literature review[J]. Head Neck Pathol, 2022, 16(3):934-941.
doi: 10.1007/s12105-022-01423-y pmid: 35257325 |
| [9] | 刘驯骅, 刘艳辉, 李智, 等. INI1缺失性鼻腔鼻窦癌9例临床病理分析[J]. 临床与实验病理学杂志, 2023, 39(3):326-330. |
| LIU X H, LIU Y H, LI Z, et al. INI1-deficient sinonasal carcinoma:clinicopathologic analysis of 9 cases and review of literatures[J]. Clin Exp Pathol, 202339(3):326-330. | |
| [10] |
KAKKAR A, ANTONY V M, PRAMANIK R, et al. SMARCB1 (INI1)-deficient sinonasal carcinoma: a series of 13 cases with assessment of histologic patterns[J]. Hum Pathol, 2019, 83:59-67.
doi: S0046-8177(18)30313-7 pmid: 30120966 |
| [11] | DERMAWAN J K, SINGER S, TAP W D, et al. The genetic landscape of SMARCB1 alterations in SMARCB1-deficient spectrum of mesenchymal neoplasms[J]. Mod Pathol, 2022, 35(12):1900-1909. |
| [12] | LI Q, ABI-SAAB T, PRILUTSKIY A, et al. Clinicopathologic and molecular characterization of SMARCB1-deificient sinonasal carcinomas -a systematic study from a single institution cohort[J]. Head Neck Pathol, 2025, 19(1):60. |
| [13] |
BANECKOVA M, COX D. Top 10 basaloid neoplasms of the sinonasal tract[J]. Head Neck Pathol, 2023, 17(1):16-32.
doi: 10.1007/s12105-022-01508-8 pmid: 36928732 |
| [14] |
XU B, KATABI N. Myoepithelial Carcinoma[J]. Surg Pathol Clin, 2021, 14(1):67-73.
doi: 10.1016/j.path.2020.09.008 pmid: 33526224 |
| [15] | SIDERIS G, SOLOMOS P, GOGOULOS P, et al. Neuroendocrine and undifferentiated sinonasal and skull base tumors: An up-to-date narrative review[J]. Oral Maxillofac Surg, 2024, 28(3):1009-1017. |
| [16] |
METE O, WENIG B M. Update from the 5th edition of the World Health Organization classification of head and neck tumors: Overview of the 2022 WHO classification of head and neck neuroendocrine neoplasms[J]. Head Neck Pathol, 2022, 16(1):123-142.
doi: 10.1007/s12105-022-01435-8 pmid: 35312985 |
| [17] | MORENO V, SALUJA K, PINA-OVIEDO S. NUT carcinoma: Clinicopathologic features, molecular genetics and epigenetics[J]. Front Oncol, 2022, 12:860830. |
| [18] | 张蕊仙, 皇甫辉, 高泽慧. SMARCB1(INI-1)缺失性鼻腔鼻窦癌的诊疗进展[J]. 中国耳鼻咽喉颅底外科杂志, 2023, 29(3):115-120. |
| ZHANG R X, HUANG F H, GAO Z H. Progress in the diagnosis and treatment of patients with SMARCB1 ( INI-1) -deficient sinonasal carcinoma[J]. Chin J Otorhinolaryngol Skull Base Surg, 2023, 29(3):115-120. | |
| [19] | SHAVERDASHVILI K, AZIMI-NEKOO E, COHEN P, et al. INI-1 (SMARCB1)-deficient undifferentiated sinonasal carcinoma: Novel paradigm of molecular testing in the diagnosis and management of sinonasal malignancies[J]. Oncologist, 2020, 25(9):738-744. |
| [20] |
WANG T, WANG J, TANG T, et al. Treatment for SMARCB1 (INI-1) deficient sinonasal tumor: a single-institution study[J]. Neoplasma, 2023, 70(6):804-810.
doi: 10.4149/neo_2023_230910N480 pmid: 38247337 |
| [21] | 王灵娃, 王茹, 房居高, 等. SMARCB1/INI-1缺失性鼻腔鼻窦癌的临床诊治分析[J]. 中华耳鼻咽喉头颈外科杂志, 2022, 57(7):848-853. |
| WANG L W, WANG R, FANG J G, et al. Analysis of the diagnosis and treatment of patients with SMARCB1 (INI-1)-deficient sinonasal carcinoma[J]. Chin J Otorhinolaryngol Head Neck Surg, 2022, 57(7):848-853. |
| [1] | SHEN Xiaonan, ZHOU Chunhua, ZHANG Benyan, GAO Lili, ZHANG Ling, HE Xiangyi, LIU Chenxiao, ZHANG Xianda, ZHANG Yao, WU Wei, GONG Tingting, ZHANG Tianyu, LIU Lei, ZOU Duowu, ZHANG Minmin. Comparative study on diagnostic performance of Acquire fine-needle biopsy and fine-needle aspiration in endoscopic ultrasonography-guided tissue acquisition for type 1 autoimmune pancreatitis [J]. Journal of Diagnostics Concepts & Practice, 2025, 24(05): 498-504. |
| [2] | ZENG Dong, SONG Shu, YANG Yuexiang, XU Jingjing, GUO Wenjuan, ZHENG Ye, SHI Yuhan, FENG Yanling. Clinicopathological features and differential diagnosis of AIDS with CMV infection [J]. Journal of Diagnostics Concepts & Practice, 2025, 24(03): 320-327. |
| [3] | GONG Jingqing, CAO Duanrong, ZHUANG Yixin, QIU Li, LI Xiaoming. Clinicopathological analysis of biphenotypic sinonasal sarcoma: a case report [J]. Journal of Diagnostics Concepts & Practice, 2025, 24(01): 100-105. |
| [4] | RUAN Miao, DA Qian, XU Haimin, DONG Lei, FEI Xiaochun. Study on clinicopathological features and prognosis of HER2 low expression breast cancer [J]. Journal of Diagnostics Concepts & Practice, 2024, 23(05): 500-508. |
| [5] | WANG Yurong, WANG Yuanyuan, WENG Haiyan. Clinical and pathological analysis of gastrointestinal leiomyosarcoma:Report of three cases [J]. Journal of Diagnostics Concepts & Practice, 2024, 23(05): 537-541. |
| [6] | NI Yaping, CHEN Yifeng, YANG Xiaoqun, CHEN Xiaoyan. Primary lung adenocarcinoma with enteroblastic differentiation: a clinicopathological and prognostic analysis of two cases [J]. Journal of Diagnostics Concepts & Practice, 2024, 23(03): 324-329. |
| [7] | XU Jiankun, ZHOU Luting, ZHANG Wenjing, XU Haimin, WANG Chaofu. The prognostic value of CA9 expression in clear cell renal cell carcinoma [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(01): 37-43. |
| [8] | WANG Zhaohui, WU Haibo. Clinicopathological analysis of 31 cases of gastric schwannoma [J]. Journal of Diagnostics Concepts & Practice, 2021, 20(06): 552-556. |
| [9] | LI Juan, LIU Jingsong, LI Mei, LI Dianwei, ZHU Hong. Bronchiolar adenoma: a clinic pathological analysis of 10 cases and review of literature [J]. Journal of Diagnostics Concepts & Practice, 2021, 20(05): 466-470. |
| [10] | WEI Ruoqu, YU Hong, YAO Zhirong. Fibroblastic connective tissue nevus in children: a case report and literature review [J]. Journal of Diagnostics Concepts & Practice, 2021, 20(02): 190-194. |
| [11] | MENG Leijun, ZHANG Jing, WANG Xueli, LI Zhi, ZHANG Hong, ZENG Naiyan. Identification of differentially expressed target genes in pediatric Burkitt lymphoma and its clinical application [J]. Journal of Diagnostics Concepts & Practice, 2020, 19(03): 248-257. |
| [12] | HE Yanyan, FENG Lijin, WEI Qing. Pleomorphic giant cell adenocarcinoma of prostate: clinicopathological analysis of a case and review of literature [J]. Journal of Diagnostics Concepts & Practice, 2019, 18(2): 160-164. |
| [13] | JIN Jiaoying, LI Qianyu, JIANG Hongwei, HAN Dongyan, XI Hao, WEI Qing. Report of a case of composite pheochromocytoma and review of literature [J]. Journal of Diagnostics Concepts & Practice, 2019, 18(2): 165-169. |
| [14] | WANG Shunli, DENG Shuangshuang, GAO Hui, XIAO Tianyu, GAO Jinli. Analysis of clinicopathological characteristics of breast encapsulated papillarycarcinoma [J]. Journal of Diagnostics Concepts & Practice, 2019, 18(1): 89-92. |
| [15] | HAN Dongyan, FU Huijun, HE Yanyan, XI Hao, WEI Qing. Endolymphatic sac tumor: Clinicopathological features and review of literature [J]. Journal of Diagnostics Concepts & Practice, 2018, 17(06): 711-714. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||