诊断学理论与实践 ›› 2024, Vol. 23 ›› Issue (02): 184-191.doi: 10.16150/j.1671-2870.2024.02.013
高梦, 柴维敏( ), 严福华
), 严福华
收稿日期:2024-03-16
出版日期:2024-04-25
发布日期:2024-07-04
通讯作者:
柴维敏 E-mail: cwm11394@rjh.com.cn
GAO Meng, CHAI Weimin(), YAN Fuhua
Received:2024-03-16
Published:2024-04-25
Online:2024-07-04
摘要:
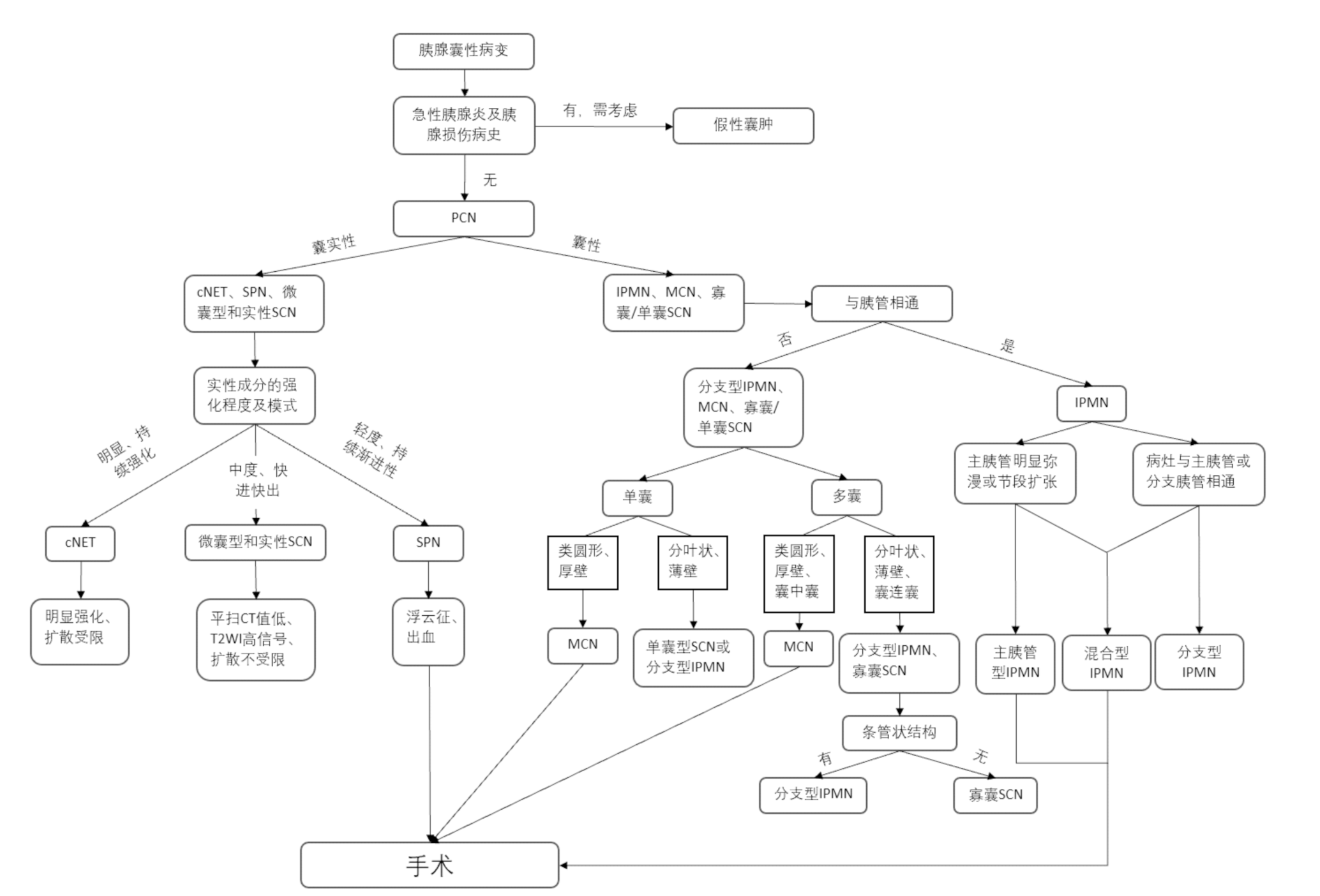
胰腺囊性肿瘤(pancreatic cystic neoplasms, PCN)是指起源于胰腺导管上皮和(或)间质组织的囊性肿瘤性病变,大致可以分为黏液性肿瘤和非黏液性肿瘤。前者主要包括导管内乳头状黏液性肿瘤(intraductal papillary mucinous neoplasm, IPMN)、黏液性囊性肿瘤(mucinous cystic neoplasm, MCN),而后者主要包括浆液性囊性肿瘤(serous cystic neoplasm, SCN)、实性假乳头状肿瘤(solid-pseudopapillary neoplasm, SPN)和囊性神经内分泌肿瘤(cystic neuroendocrine tumor, cNET)。不同类型的PCN具有差异化的生物学行为,部分PCN存在恶变的风险,术前采用CT、MRI检查鉴别恶性肿瘤具有重要意义。MCN恶变率为5%~20%,恶性指征为直径大于等于4 cm,为手术指征。IPMN占PCN的22%,主胰管型及混合型IPMN恶变风险可高达70.9%和76.5%,分支胰管型IPMN的恶变风险为2.8%~10.7%。IPMN高危征象包括,强化的实质成分或壁结节直径≥5 mm、主胰管扩张(管径≥10 mm)、梗阻性黄疸,并推荐这些患者行手术治疗。SCN好发于中老年女性,男女比例为1:3,多为良性,浆液性囊腺癌罕见,仅占胰腺SCN的0.1%。2015版胰腺囊性疾病诊治指南推荐,所有的SPN均应行手术治疗。当SPN肿瘤包膜不完整、肿块直径大于6 cm或位于胰尾部可能具有较高的侵袭性和远处转移能力。cNET约占PCN的7%。PCN影像学诊断需结合病史及病变成分等,诊断要点为,MCN为几乎均发生于女性的胰体尾部类圆形、厚壁囊性肿瘤,常呈“囊内囊”表现;IPMN好发于老年男性,主胰管型IPMN表现为除外梗阻性因素的主胰管弥漫性明显扩张或节段性扩张,分支胰管型IPMN通常表现为与胰管相通的条管状囊性肿瘤,混合型IPMN则兼有两者表现;SCN为分叶状、薄壁寡囊或多囊蜂窝状肿瘤;SPN为好发于青年女性的较大类圆形囊实性肿瘤;cNET为边缘呈环形或新月形明显强化的囊实性肿瘤。国内外指南关于PCN手术指征的选择存在较大争议,且胰腺手术难度高、术后并发症多,给PCN的规范化治疗带来了挑战。识别PCN的影像学特点,明确影像学诊断,具有临床意义。
中图分类号:
高梦, 柴维敏, 严福华. 胰腺囊性肿瘤的CT/MRI诊断进展[J]. 诊断学理论与实践, 2024, 23(02): 184-191.
GAO Meng, CHAI Weimin, YAN Fuhua. Advance in study on diagnosis of pancreatic cystic tumors on CT/MRI imaging[J]. Journal of Diagnostics Concepts & Practice, 2024, 23(02): 184-191.

图1
MCN(28岁,女性)


图2
主胰管型IPMN(77岁,男性)
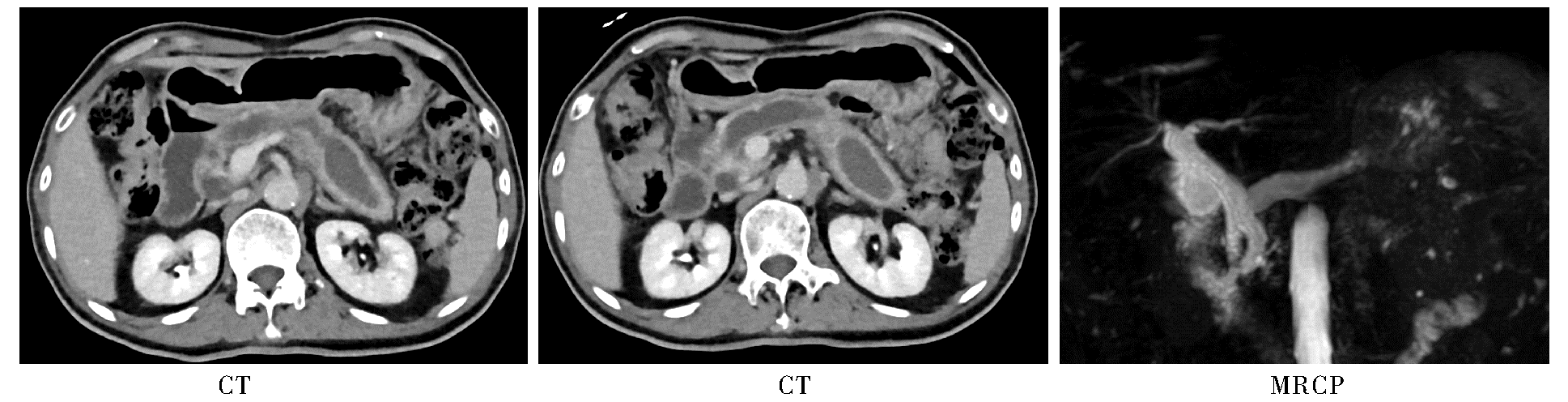
图3
分支胰管型IPMN(55岁,女性)
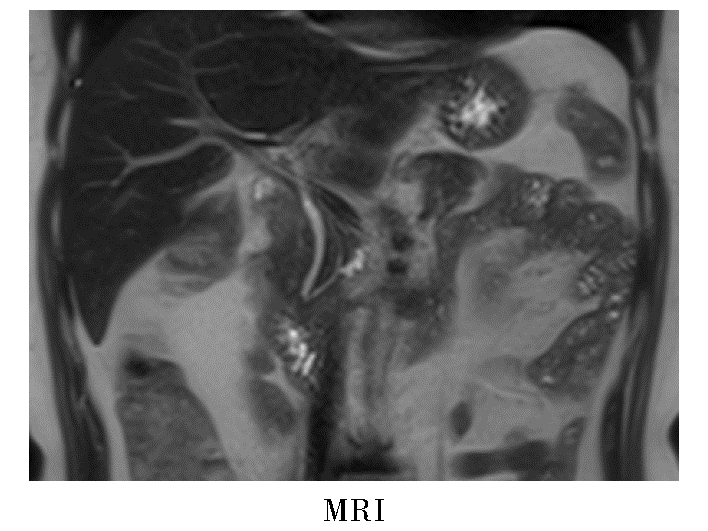
图4
混合型IPMN(79岁,男性)
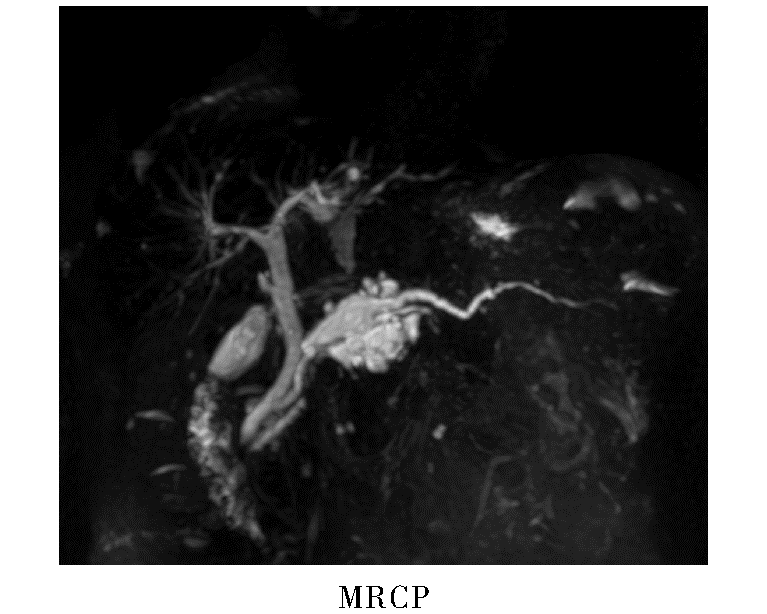
图5
SCN(53岁,女性)


图6
SPN(37岁,女性)

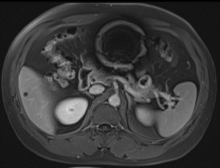
图7
cNET(38岁,男性)
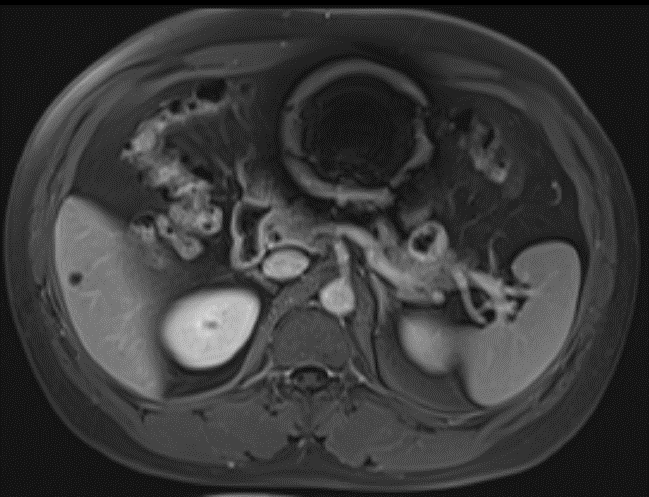
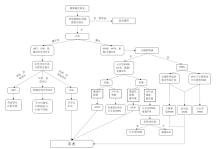
图8
胰腺囊性肿瘤CT/MRI诊断思路流程图(手术指征参照2015版胰腺囊性疾病诊治指南)
| [1] | SCHUBACH A, KOTHARI S, KOTHARI T. Pancreatic cystic neoplasms: diagnosis and management[J]. Diagnostics (Basel), 2023, 13(2):207. |
| [2] | KROMREY M L, BÜLOW R, HÜBNER J, et al. Prospective study on the incidence, prevalence and 5-year pancreatic-related mortality of pancreatic cysts in a population-based study[J]. Gut, 2018, 67(1):138-145. |
| [3] |
NAGTEGAAL I D, ODZE R D, KLIMSTRA D, et al. The 2019 WHO classification of tumours of the digestive system[J]. Histopathology, 2020, 76(2):182-188.
doi: 10.1111/his.13975 pmid: 31433515 |
| [4] | 中华医学会外科学分会胰腺外科学组. 胰腺囊性疾病诊治指南(2015版)[J]. 中华消化外科杂志, 2015, 14(9):689-693. |
| Pancreatic Surgery Group of Surgery Branch of Chinese Medical Association. Guideline for the diagnosis and treatment of pancreatic cystic diseases (2015 edition)[J]. Chin J Dig Surg, 2015, 14(9):689-693. | |
| [5] | 张太平, 刘悦泽, 邱江东, 等. 胰腺囊性肿瘤临床诊断与治疗指南的进展与比较[J]. 中华消化外科杂志, 2020, 19(4):374-378. |
| ZHANG T P, LIU Y Z, QIU J D, et al. Advances in and comparison between related clinical guidelines for diagnosis and treatment of pancreatic cystic neoplasm[J]. Chin J Dig Surg, 2020, 19(4):374-378. | |
| [6] | LUK L, LOWY A M, LI K, et al. Pancreatic cyst surveillance: Who, why, how?[J]. Radiology, 2023, 308(1):e222778. |
| [7] | 李兆申, 金震东, 李汛. 中国胰腺囊性肿瘤诊断指南(2022年)[J]. 临床肝胆病杂志, 2023, 39(2):290-298. |
| LI Z S, JIN Z D, LI X. Chinese guidelines for the diagnosis and treatment of pancrestic cystic neoplasm(2022)[J]. J Clin Hepatol, 2023, 39(2):290-298. | |
| [8] |
CRIPPA S, SALVIA R, WARSHAW A L, et al. Mucinous cystic neoplasm of the pancreas is not an aggressive entity: lessons from 163 resected patients[J]. Ann Surg, 2008, 247(4):571-579.
doi: 10.1097/SLA.0b013e31811f4449 pmid: 18362619 |
| [9] | XIE W, LIANG H Y, GUO Y, et al. Update on mucinous cystic neoplasm of the pancreas: a narrative review[J]. J Pancreatol, 2021, 4(3) : 115-121. |
| [10] |
NILSSON L N, KEANE M G, SHAMALI A, et al. Nature and management of pancreatic mucinous cystic neoplasm (MCN): A systematic review of the literature[J]. Pancreatology, 2016, 16(6):1028-1036.
doi: S1424-3903(16)31208-X pmid: 27681503 |
| [11] | MORMUL A, WŁOSZEK E, NOWOSZEWSKA J, et al. Rare non-neuroendocrine pancreatic tumours[J]. Cancers (Basel), 2023, 15(8):2216. |
| [12] | COHEN-SCALI F, VILGRAIN V, BRANCATELLI G, et al. Discrimination of unilocular macrocystic serous cystadenoma from pancreatic pseudocyst and mucinous cystadenoma with CT: initial observations[J]. Radiology, 2003, 228(3):727-733. |
| [13] | MANFREDI R, VENTRIGLIA A, MANTOVANI W, et al. Mucinous cystic neoplasms and serous cystadenomas arising in the body-tail of the pancreas: MR imaging chara-cterization[J]. Eur Radiol, 2015, 25(4):940-949. |
| [14] | VULLIERME M P, GREGORY J, REBOURS V, et al. MRI is useful to suggest and exclude malignancy in mucinous cystic neoplasms of the pancreas[J]. Eur Radiol, 2022, 32(2):1297-1307. |
| [15] | KIM S Y, LEE J M, KIM S H, et al. Macrocystic neoplasms of the pancreas: CT differentiation of serous oligocystic adenoma from mucinous cystadenoma and intraductal papillary mucinous tumor[J]. AJR Am J Roentgenol, 2006, 187(5):1192-1198. |
| [16] |
MAMONE G, BARRESI L, TROPEA A, et al. MRI of mucinous pancreatic cystic lesions: a new updated morphological approach for the differential diagnosis[J]. Updates Surg, 2020, 72(3):617-637.
doi: 10.1007/s13304-020-00800-y pmid: 32462610 |
| [17] | SERVIN-ROJAS M, FONG Z V, FERNANDEZ-DEL CASTILLO C, et al. Identification of high-risk features in mucinous cystic neoplasms of the pancreas[J]. Surgery, 2023, 173(5):1270-1274. |
| [18] |
European Study Group on Cystic Tumours of the Pancreas. European evidence-based guidelines on pancreatic cystic neoplasms[J]. Gut. 2018; 67(5):789-804.
doi: 10.1136/gutjnl-2018-316027 pmid: 29574408 |
| [19] | 中华外科青年医师学术研究社胰腺外科研究组. 中国胰腺囊性肿瘤外科诊治现状分析:2251例报告[J]. 中华外科杂志, 2018, 56(1):24-29. |
| Pancreatic Surgery of Chinese Academic Society of Young Surgeons. The current status of diagnosis and treatment of pancreatic cystic neoplasm in China: a report of 2 251 cases[J]. Chin J Surg, 2018, 56(1):24-29. | |
| [20] | FUJITA Y, HIRONO S, KAWAI M, et al. Malignant potential and specific characteristics of pure main duct type intraductal papillary mucinous neoplasm[J]. Eur J Surg Oncol, 2022, 48(5):1054-1061. |
| [21] | 楼文晖, 赵玉沛. 重视胰腺囊性肿瘤诊治过程中存在的问题[J]. 中华外科杂志, 2018, 56(1):2-4. |
| LOU W H, ZHAO Y P. Important issues need to be emphasized in the diagnosis and treatment of pancreatic cystic neoplasms[J]. Chin J Surg, 2018, 56(1):2-4. | |
| [22] | 王鑫, 方旭, 边云, 等. 胰腺浆液性囊性肿瘤伴胰管扩张患者的影像学误诊情况分析[J]. 中华肝胆外科杂志, 2022, 28(7):510-514. |
| WANG X, FANG X, BIAN Y, et al. Medical imaging in misdiagnosing serous cystic neoplasms of the pancreas with pancreatic duct dilatation as other pancreatic lessions[J]. Chin J Hepatobiliary Surg, 2022, 28(7):510-514. | |
| [23] | HU F, HU Y, WANG D, et al. Cystic neoplasms of the pancreas: differential diagnosis and radiology correlation[J]. Front Oncol, 2022, 12:860740. |
| [24] | 阮志兵, 焦俊, 瞿金环, 等. 胰头部肿块型慢性胰腺炎与胰头癌的多模态影像学鉴别诊断[J]. 临床放射学杂志, 2019, 38(1):88-94. |
| RUAN Z B, JIAO J, QU J H, et al. The clinical value of multi-modality imaging in differentiating pancreatic ductal carcinoma from the mass-forming chronic pancreatitis of the pancreatic head[J]. J of Clin Radiol, 2019, 38(1):88-94. | |
| [25] | MARCHEGIANI G, POLLINI T, BURELLI A, et al. Surveillance for presumed BD-IPMN of the pancreas: stabi-lity, size, and age identify targets for discontinuation[J]. Gastroenterology, 2023, 165(4):1016-1024.e5. |
| [26] | TRIANTOPOULOU C, GOURTSOYIANNI S, KARAKAXAS D, et al. Intraductal papillary mucinous neoplasm of the pancreas: a challenging diagnosis[J]. Diagnostics (Basel), 2023, 13(12):2015. |
| [27] | BORASCHI P, DONATI F, GIGONI R, et al. Diffusion-weighted MRI in the characterization of cystic pancreatic lesions: usefulness of ADC values[J]. Magn Reson Imagi-ng, 2010, 28(10):1447-1455. |
| [28] |
BORASCHI P, SCALISE P, CASOTTI M T, et al. Cystic lesions of the pancreas: is apparent diffusion coefficient value useful at 3 T magnetic resonance imaging?[J]. J Comput Assist Tomogr, 2022, 46(3):363-370.
doi: 10.1097/RCT.0000000000001302 pmid: 35405726 |
| [29] |
TANAKA M, FERNÁNDEZ-DEL CASTILLO C, KAMISAWA T, et al. Revisions of international consensus Fukuoka guidelines for the management of IPMN of the pancreas[J]. Pancreatology, 2017, 17(5):738-753.
doi: S1424-3903(17)30516-1 pmid: 28735806 |
| [30] |
JAIS B, REBOURS V, MALLEO G, et al. Serous cystic neoplasm of the pancreas: a multinational study of 2622 patients under the auspices of the International Association of Pancreatology and European Pancreatic Club (European Study Group on Cystic Tumors of the Pancreas)[J]. Gut, 2016, 65(2):305-312.
doi: 10.1136/gutjnl-2015-309638 pmid: 26045140 |
| [31] | CHU L C, SINGHI A D, HAROUN R R, et al. The many faces of pancreatic serous cystadenoma: Radiologic and pathologic correlation[J]. Diagn Interv Imaging, 2017, 98(3):191-202. |
| [32] | 张宏艳, 王志锋, 马小龙, 等. 胰腺浆液性囊腺瘤的影像学类型与病理对照[J]. 放射学实践, 2015(7):768-771. |
| ZHANG H Y, WANG Z F, MA X L, et al. Serous cysta-denoma of the pancreas:a comparative study of imaging types and pathological features[J]. Radiol Pract, 2015, 30(7):768-771. | |
| [33] | 王晴柔, 陈克敏, 朱兰, 等. MDCT在鉴别胰腺实性型浆液性囊腺瘤与富血供神经内分泌肿瘤中的价值[J]. 中国医学计算机成像杂志, 2022, 28(1):50-55. |
| WANG Q R, CHEN K M, ZHU L, et al. MDCT in diffe-rentiation of solid serous cystadenoma and hypervascular neuroendocrine tumor of the pancreas[J]. Chin Comput Med Imag, 2022, 28(1):50-55. | |
| [34] |
PARK H S, KIM S Y, HONG S M, et al. Hypervascular solid-appearing serous cystic neoplasms of the pancreas: Differential diagnosis with neuroendocrine tumours[J]. Eur Radiol, 2016, 26(5):1348-1358.
doi: 10.1007/s00330-015-3961-3 pmid: 26328927 |
| [35] | LAW J K, AHMED A, SINGH V K, et al. A systematic review of solid-pseudopapillary neoplasms: are these rare lesions?[J]. Pancreas, 2014, 43(3):331-337. |
| [36] | 龚毅, 汪晓红, 张盛箭, 等. 胰腺实性假乳头状肿瘤的影像特征分析[J]. 放射学实践, 2020, 35(1):56-60. |
| GONG Y, WANG X H, ZHANG S J, et al. Imaging features analysis of pancreatic solid pseudopapillary tumor[J]. Radiol Pract, 2020, 35(1):56-60. | |
| [37] | 计凤鸣, 王连敏, 丁珏宁君, 等. 胰腺实性假乳头状瘤的临床研究进展[J]. 医学综述, 2019, 25(5):909-914, 921. |
| JI F M, WANG L M, DING Y N J, et al. Progress in clinical research of solid pseudopapillary tumor of pancreas[J]. Med Recapitulate, 2019, 25(5):909-914, 921. | |
| [38] |
YU P, CHENG X, DU Y, et al. Solid pseudopapillary neoplasms of the pancreas: a 19-year multicenter experience in China[J]. J Gastrointest Surg, 2015, 19(8):1433-1440.
doi: 10.1007/s11605-015-2862-8 pmid: 26001371 |
| [39] |
YIN Q, WANG M, WANG C, et al. Differentiation between benign and malignant solid pseudopapillary tumor of the pancreas by MDCT[J]. Eur J Radiol, 2012, 81(11):3010-3018.
doi: 10.1016/j.ejrad.2012.03.013 pmid: 22520082 |
| [40] | VALSANGKAR N P, MORALES-OYARVIDE V, THAYER S P, et al. 851 resected cystic tumors of the pancreas: a 33-year experience at the Massachusetts General Hospital[J]. Surgery, 2012, 152(3 Suppl 1):S4-S12. |
| [41] | 张育森, 鲍世韵, 孙枫林, 等. 胰腺囊性肿瘤39例临床分析[J]. 中国医药导报, 2015(20):101-104. |
| ZHANG Y S, BAO S Y, SUN F L, et al. Clinical analysis of 39 cases with pancreatic cystic neoplasms[J]. Chin Med Herald, 2015, 12(20):101-104. | |
| [42] | CAGLIÀ P, CANNIZZARO M T, TRACIA A, et al. Cystic pancreatic neuroendocrine tumors: To date a diagnostic challenge[J]. Int J Surg, 2015, 21 Suppl 1:S44-S49. |
| [43] | 王慧, 李楠, 张艺璇, 等. 超声内镜下细针穿刺术对胰腺囊性神经内分泌肿瘤的诊断价值[J]. 中华胰腺病杂志, 2020, 20(5):386-388. |
| WANG H, LI N, ZHANG Y X, et al. The diagnostic value of EUS-FNA for pancreatic cystic neuroendocrine tumors[J]. Chin J Pancreatol, 2020, 20(5):386-388. | |
| [44] | KAWAMOTO S, JOHNSON P T, SHI C, et al. Pancreatic neuroendocrine tumor with cystlike changes: evaluation with MDCT[J]. Am J Roentgenol, 2013, 200(3):W283-W290. |
| [45] |
BAIOCCHI G L, PORTOLANI N, MISSALE G, et al. Intraductal papillary mucinous neoplasm of the pancreas (IPMN): clinico-pathological correlations and surgical indications[J]. World J Surg Oncol, 2010, 8:25.
doi: 10.1186/1477-7819-8-25 pmid: 20374620 |
| [1] | 查云飞, 武夏夏. MRI深度学习图像重建技术在肌骨系统疾病诊断的应用进展[J]. 诊断学理论与实践, 2024, 23(02): 114-118. |
| [2] | 李明, 陈克敏, 潘自来, 罗禹. CT及MRI预测急性缺血性脑梗死出血性转化的价值研究进展[J]. 诊断学理论与实践, 2024, 23(01): 83-89. |
| [3] | 丁景峰, 敖炜群, 朱珍, 孙静, 徐良根, 郑世保, 俞晶晶, 胡金文. 基于T2WI和DWI的磁共振影像组学在术前预测直肠癌壁外血管侵犯的价值研究[J]. 诊断学理论与实践, 2024, 23(01): 46-56. |
| [4] | 周熠磊, 张淼, 郭睿, 周金鑫, 李彪, 李翔. 18F-PSMA PET/MRI在早期诊断前列腺癌根治术后复发、转移中的价值[J]. 诊断学理论与实践, 2023, 22(06): 567-572. |
| [5] | 冯丽, 任刚, 蔡嵘, 汪心韵, 王辉, 祝明洁. 泌尿生殖系统血管周上皮样细胞瘤(PEComa)的临床特征分析[J]. 诊断学理论与实践, 2023, 22(05): 460-465. |
| [6] | 李笑石, 秦越. 影像学技术在痛风诊断及疾病监测中的应用研究进展[J]. 诊断学理论与实践, 2023, 22(03): 311-318. |
| [7] | 李卫侠, 徐学勤, 朱晓雷, 陈克敏. 39例肾上腺皮质癌患者的CT、MRI影像特点及其诊断价值[J]. 诊断学理论与实践, 2023, 22(02): 134-140. |
| [8] | 陈乾, 林慧敏, 严福华. 磁共振成像评估肝功能储备的研究进展[J]. 诊断学理论与实践, 2023, 22(02): 190-196. |
| [9] | 黄娟, 朱晓雷, 李晓, 陈克敏, 严福华, 徐学勤. 血氧水平依赖磁共振成像评估早期慢性肾病肾缺氧的研究[J]. 诊断学理论与实践, 2022, 21(03): 385-389. |
| [10] | 朱乃懿, 姜奕歆, 柴丽, 柴维敏. 磁共振对超声阴性而乳腺X线检出BI-RADS4类以上钙化灶的诊断价值分析[J]. 诊断学理论与实践, 2021, 20(05): 439-444. |
| [11] | 张雪坤, 李彦, 严福华, 赵洪飞, 宋琦. 基于光梭成像的新型加速技术在颅脑MRI中的应用价值研究[J]. 诊断学理论与实践, 2021, 20(04): 378-383. |
| [12] | 孙甜甜, 叶宝英, 杨钰, 牛建梅. 彩色多普勒超声与磁共振成像在凶险型前置胎盘及合并胎盘植入产前诊断中的应用及漏诊分析[J]. 诊断学理论与实践, 2021, 20(02): 173-177. |
| [13] | 曹琪琪, 秦乐, 周慧娟, 杨之涛, 苏文婷, 杨文洁, 程增辉, 陆勇, 严福华, 潘自来. 新型冠状病毒(2019-nCoV)肺炎的CT征象分析[J]. 诊断学理论与实践, 2020, 19(1): 16-19. |
| [14] | 吴霜, 解骞, 管雪妮, 张素芳, 高信芳, 梁宗辉. 磁共振体素内不相干运动扩散加权成像诊断活动期克罗恩病的价值及效能分析[J]. 诊断学理论与实践, 2020, 19(02): 157-161. |
| [15] | 王兰, 张欢, 葛颖倩, 陆静, 崔征, 颜凌, 潘自来. 胃癌肝转移病灶的人工智能辅助半自动分割软件的临床应用评估[J]. 诊断学理论与实践, 2019, 18(05): 515-520. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||