Journal of Diagnostics Concepts & Practice ›› 2024, Vol. 23 ›› Issue (02): 184-191.doi: 10.16150/j.1671-2870.2024.02.013
• Review articles • Previous Articles Next Articles
GAO Meng, CHAI Weimin( ), YAN Fuhua
), YAN Fuhua
Received:2024-03-16
Online:2024-04-25
Published:2024-07-04
Contact:
CHAI Weimin
E-mail:cwm11394@rjh.com.cn
CLC Number:
GAO Meng, CHAI Weimin, YAN Fuhua. Advance in study on diagnosis of pancreatic cystic tumors on CT/MRI imaging[J]. Journal of Diagnostics Concepts & Practice, 2024, 23(02): 184-191.

Figure 1
MCN(28 years old, female)


Figure 2
Main pancreatic duct type of IPMN(77 years old, male)
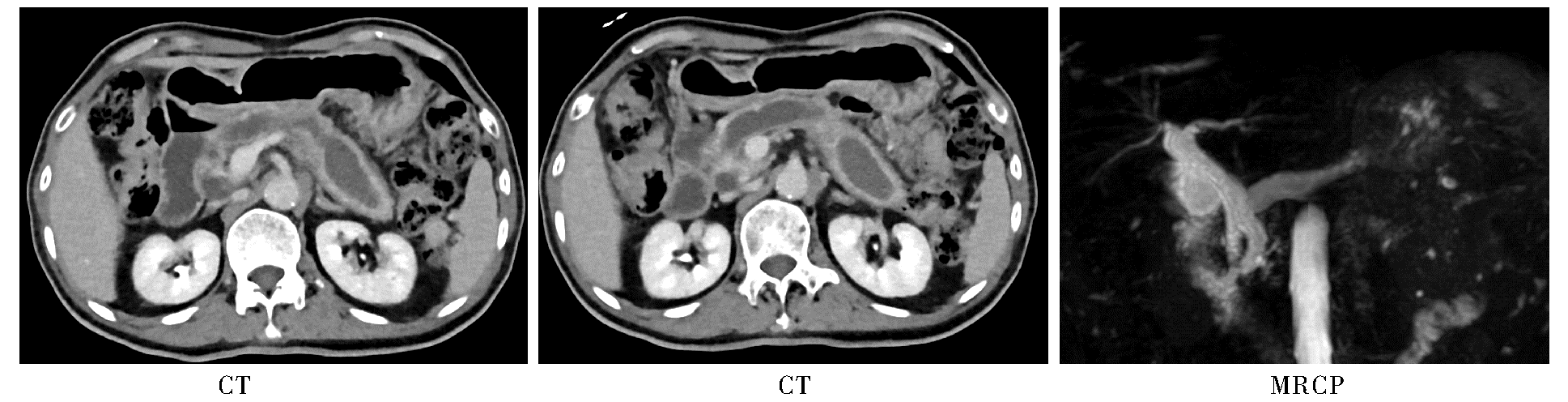
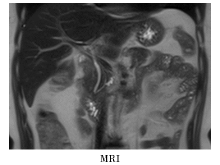
Figure 3
Branch pancreatic duct type of IPMN(55 years old, female)
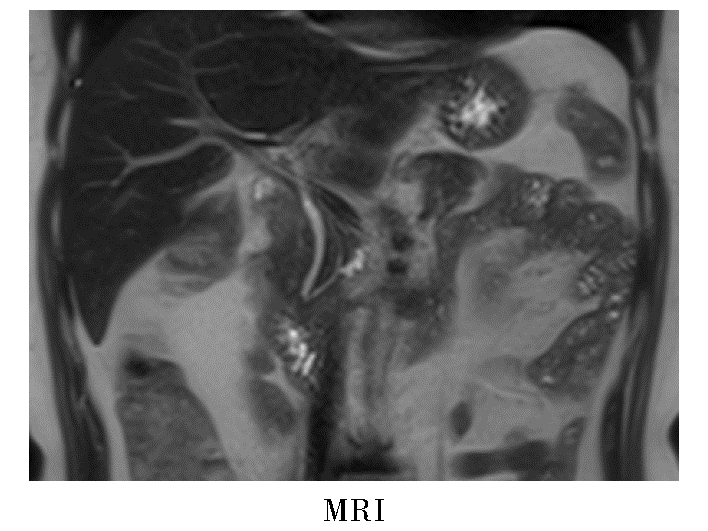
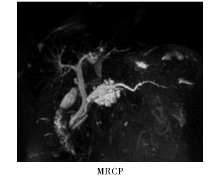
Figure 4
Mixed type of IPMN(79 years old, male)
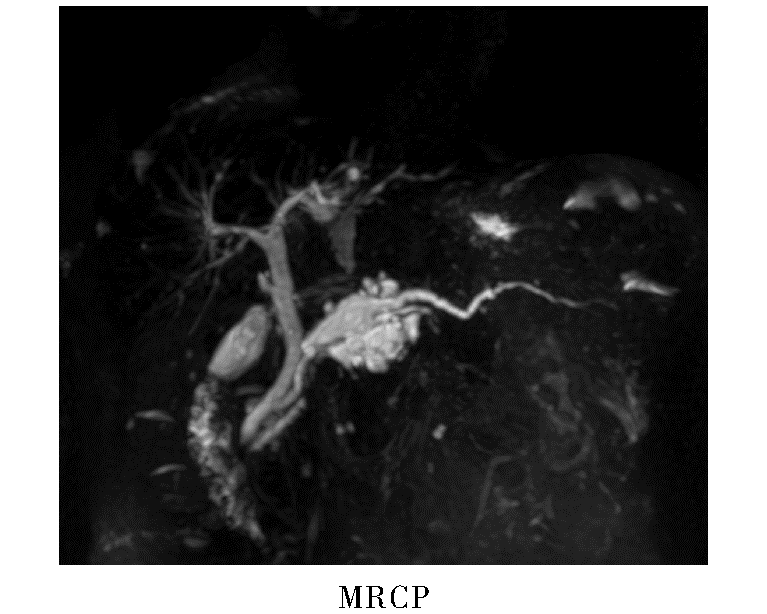
Figure 5
SCN(53 years old, female)


Figure 6
SPN(37 years old, female)

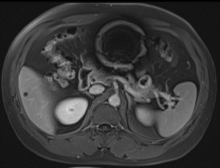
Figure 7
cNET(38 years old, male)
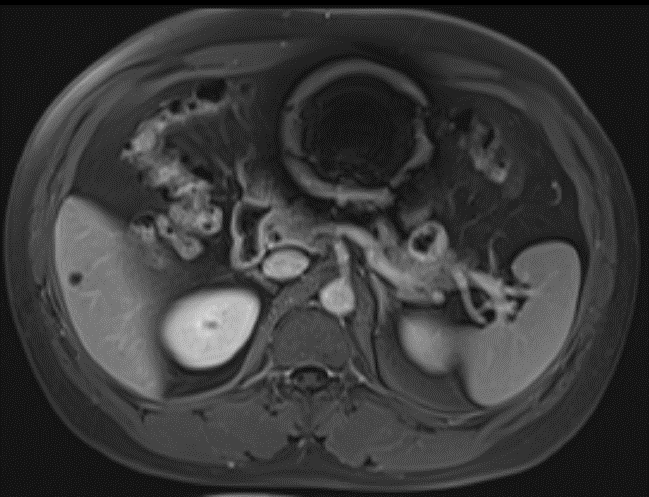
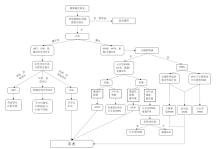
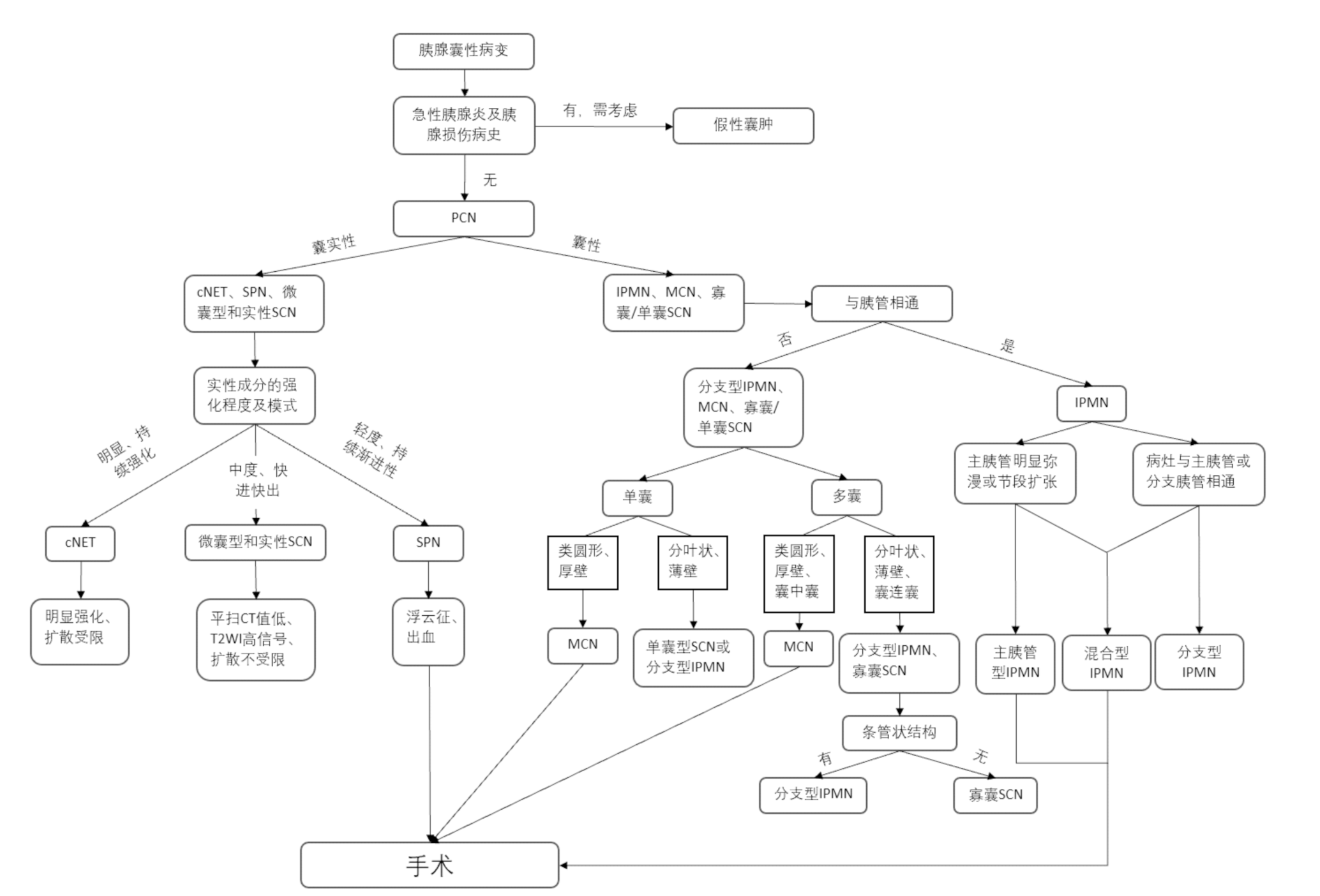
Figure 8
CT/MRI diagnosis for pancreatic cystic neoplasms (surgical indications refer to the 2015 edition of the Diagnosis and Treatment Guidelines for Pancreatic Cystic Diseases)
| [1] | SCHUBACH A, KOTHARI S, KOTHARI T. Pancreatic cystic neoplasms: diagnosis and management[J]. Diagnostics (Basel), 2023, 13(2):207. |
| [2] | KROMREY M L, BÜLOW R, HÜBNER J, et al. Prospective study on the incidence, prevalence and 5-year pancreatic-related mortality of pancreatic cysts in a population-based study[J]. Gut, 2018, 67(1):138-145. |
| [3] |
NAGTEGAAL I D, ODZE R D, KLIMSTRA D, et al. The 2019 WHO classification of tumours of the digestive system[J]. Histopathology, 2020, 76(2):182-188.
doi: 10.1111/his.13975 pmid: 31433515 |
| [4] | 中华医学会外科学分会胰腺外科学组. 胰腺囊性疾病诊治指南(2015版)[J]. 中华消化外科杂志, 2015, 14(9):689-693. |
| Pancreatic Surgery Group of Surgery Branch of Chinese Medical Association. Guideline for the diagnosis and treatment of pancreatic cystic diseases (2015 edition)[J]. Chin J Dig Surg, 2015, 14(9):689-693. | |
| [5] | 张太平, 刘悦泽, 邱江东, 等. 胰腺囊性肿瘤临床诊断与治疗指南的进展与比较[J]. 中华消化外科杂志, 2020, 19(4):374-378. |
| ZHANG T P, LIU Y Z, QIU J D, et al. Advances in and comparison between related clinical guidelines for diagnosis and treatment of pancreatic cystic neoplasm[J]. Chin J Dig Surg, 2020, 19(4):374-378. | |
| [6] | LUK L, LOWY A M, LI K, et al. Pancreatic cyst surveillance: Who, why, how?[J]. Radiology, 2023, 308(1):e222778. |
| [7] | 李兆申, 金震东, 李汛. 中国胰腺囊性肿瘤诊断指南(2022年)[J]. 临床肝胆病杂志, 2023, 39(2):290-298. |
| LI Z S, JIN Z D, LI X. Chinese guidelines for the diagnosis and treatment of pancrestic cystic neoplasm(2022)[J]. J Clin Hepatol, 2023, 39(2):290-298. | |
| [8] |
CRIPPA S, SALVIA R, WARSHAW A L, et al. Mucinous cystic neoplasm of the pancreas is not an aggressive entity: lessons from 163 resected patients[J]. Ann Surg, 2008, 247(4):571-579.
doi: 10.1097/SLA.0b013e31811f4449 pmid: 18362619 |
| [9] | XIE W, LIANG H Y, GUO Y, et al. Update on mucinous cystic neoplasm of the pancreas: a narrative review[J]. J Pancreatol, 2021, 4(3) : 115-121. |
| [10] |
NILSSON L N, KEANE M G, SHAMALI A, et al. Nature and management of pancreatic mucinous cystic neoplasm (MCN): A systematic review of the literature[J]. Pancreatology, 2016, 16(6):1028-1036.
doi: S1424-3903(16)31208-X pmid: 27681503 |
| [11] | MORMUL A, WŁOSZEK E, NOWOSZEWSKA J, et al. Rare non-neuroendocrine pancreatic tumours[J]. Cancers (Basel), 2023, 15(8):2216. |
| [12] | COHEN-SCALI F, VILGRAIN V, BRANCATELLI G, et al. Discrimination of unilocular macrocystic serous cystadenoma from pancreatic pseudocyst and mucinous cystadenoma with CT: initial observations[J]. Radiology, 2003, 228(3):727-733. |
| [13] | MANFREDI R, VENTRIGLIA A, MANTOVANI W, et al. Mucinous cystic neoplasms and serous cystadenomas arising in the body-tail of the pancreas: MR imaging chara-cterization[J]. Eur Radiol, 2015, 25(4):940-949. |
| [14] | VULLIERME M P, GREGORY J, REBOURS V, et al. MRI is useful to suggest and exclude malignancy in mucinous cystic neoplasms of the pancreas[J]. Eur Radiol, 2022, 32(2):1297-1307. |
| [15] | KIM S Y, LEE J M, KIM S H, et al. Macrocystic neoplasms of the pancreas: CT differentiation of serous oligocystic adenoma from mucinous cystadenoma and intraductal papillary mucinous tumor[J]. AJR Am J Roentgenol, 2006, 187(5):1192-1198. |
| [16] |
MAMONE G, BARRESI L, TROPEA A, et al. MRI of mucinous pancreatic cystic lesions: a new updated morphological approach for the differential diagnosis[J]. Updates Surg, 2020, 72(3):617-637.
doi: 10.1007/s13304-020-00800-y pmid: 32462610 |
| [17] | SERVIN-ROJAS M, FONG Z V, FERNANDEZ-DEL CASTILLO C, et al. Identification of high-risk features in mucinous cystic neoplasms of the pancreas[J]. Surgery, 2023, 173(5):1270-1274. |
| [18] |
European Study Group on Cystic Tumours of the Pancreas. European evidence-based guidelines on pancreatic cystic neoplasms[J]. Gut. 2018; 67(5):789-804.
doi: 10.1136/gutjnl-2018-316027 pmid: 29574408 |
| [19] | 中华外科青年医师学术研究社胰腺外科研究组. 中国胰腺囊性肿瘤外科诊治现状分析:2251例报告[J]. 中华外科杂志, 2018, 56(1):24-29. |
| Pancreatic Surgery of Chinese Academic Society of Young Surgeons. The current status of diagnosis and treatment of pancreatic cystic neoplasm in China: a report of 2 251 cases[J]. Chin J Surg, 2018, 56(1):24-29. | |
| [20] | FUJITA Y, HIRONO S, KAWAI M, et al. Malignant potential and specific characteristics of pure main duct type intraductal papillary mucinous neoplasm[J]. Eur J Surg Oncol, 2022, 48(5):1054-1061. |
| [21] | 楼文晖, 赵玉沛. 重视胰腺囊性肿瘤诊治过程中存在的问题[J]. 中华外科杂志, 2018, 56(1):2-4. |
| LOU W H, ZHAO Y P. Important issues need to be emphasized in the diagnosis and treatment of pancreatic cystic neoplasms[J]. Chin J Surg, 2018, 56(1):2-4. | |
| [22] | 王鑫, 方旭, 边云, 等. 胰腺浆液性囊性肿瘤伴胰管扩张患者的影像学误诊情况分析[J]. 中华肝胆外科杂志, 2022, 28(7):510-514. |
| WANG X, FANG X, BIAN Y, et al. Medical imaging in misdiagnosing serous cystic neoplasms of the pancreas with pancreatic duct dilatation as other pancreatic lessions[J]. Chin J Hepatobiliary Surg, 2022, 28(7):510-514. | |
| [23] | HU F, HU Y, WANG D, et al. Cystic neoplasms of the pancreas: differential diagnosis and radiology correlation[J]. Front Oncol, 2022, 12:860740. |
| [24] | 阮志兵, 焦俊, 瞿金环, 等. 胰头部肿块型慢性胰腺炎与胰头癌的多模态影像学鉴别诊断[J]. 临床放射学杂志, 2019, 38(1):88-94. |
| RUAN Z B, JIAO J, QU J H, et al. The clinical value of multi-modality imaging in differentiating pancreatic ductal carcinoma from the mass-forming chronic pancreatitis of the pancreatic head[J]. J of Clin Radiol, 2019, 38(1):88-94. | |
| [25] | MARCHEGIANI G, POLLINI T, BURELLI A, et al. Surveillance for presumed BD-IPMN of the pancreas: stabi-lity, size, and age identify targets for discontinuation[J]. Gastroenterology, 2023, 165(4):1016-1024.e5. |
| [26] | TRIANTOPOULOU C, GOURTSOYIANNI S, KARAKAXAS D, et al. Intraductal papillary mucinous neoplasm of the pancreas: a challenging diagnosis[J]. Diagnostics (Basel), 2023, 13(12):2015. |
| [27] | BORASCHI P, DONATI F, GIGONI R, et al. Diffusion-weighted MRI in the characterization of cystic pancreatic lesions: usefulness of ADC values[J]. Magn Reson Imagi-ng, 2010, 28(10):1447-1455. |
| [28] |
BORASCHI P, SCALISE P, CASOTTI M T, et al. Cystic lesions of the pancreas: is apparent diffusion coefficient value useful at 3 T magnetic resonance imaging?[J]. J Comput Assist Tomogr, 2022, 46(3):363-370.
doi: 10.1097/RCT.0000000000001302 pmid: 35405726 |
| [29] |
TANAKA M, FERNÁNDEZ-DEL CASTILLO C, KAMISAWA T, et al. Revisions of international consensus Fukuoka guidelines for the management of IPMN of the pancreas[J]. Pancreatology, 2017, 17(5):738-753.
doi: S1424-3903(17)30516-1 pmid: 28735806 |
| [30] |
JAIS B, REBOURS V, MALLEO G, et al. Serous cystic neoplasm of the pancreas: a multinational study of 2622 patients under the auspices of the International Association of Pancreatology and European Pancreatic Club (European Study Group on Cystic Tumors of the Pancreas)[J]. Gut, 2016, 65(2):305-312.
doi: 10.1136/gutjnl-2015-309638 pmid: 26045140 |
| [31] | CHU L C, SINGHI A D, HAROUN R R, et al. The many faces of pancreatic serous cystadenoma: Radiologic and pathologic correlation[J]. Diagn Interv Imaging, 2017, 98(3):191-202. |
| [32] | 张宏艳, 王志锋, 马小龙, 等. 胰腺浆液性囊腺瘤的影像学类型与病理对照[J]. 放射学实践, 2015(7):768-771. |
| ZHANG H Y, WANG Z F, MA X L, et al. Serous cysta-denoma of the pancreas:a comparative study of imaging types and pathological features[J]. Radiol Pract, 2015, 30(7):768-771. | |
| [33] | 王晴柔, 陈克敏, 朱兰, 等. MDCT在鉴别胰腺实性型浆液性囊腺瘤与富血供神经内分泌肿瘤中的价值[J]. 中国医学计算机成像杂志, 2022, 28(1):50-55. |
| WANG Q R, CHEN K M, ZHU L, et al. MDCT in diffe-rentiation of solid serous cystadenoma and hypervascular neuroendocrine tumor of the pancreas[J]. Chin Comput Med Imag, 2022, 28(1):50-55. | |
| [34] |
PARK H S, KIM S Y, HONG S M, et al. Hypervascular solid-appearing serous cystic neoplasms of the pancreas: Differential diagnosis with neuroendocrine tumours[J]. Eur Radiol, 2016, 26(5):1348-1358.
doi: 10.1007/s00330-015-3961-3 pmid: 26328927 |
| [35] | LAW J K, AHMED A, SINGH V K, et al. A systematic review of solid-pseudopapillary neoplasms: are these rare lesions?[J]. Pancreas, 2014, 43(3):331-337. |
| [36] | 龚毅, 汪晓红, 张盛箭, 等. 胰腺实性假乳头状肿瘤的影像特征分析[J]. 放射学实践, 2020, 35(1):56-60. |
| GONG Y, WANG X H, ZHANG S J, et al. Imaging features analysis of pancreatic solid pseudopapillary tumor[J]. Radiol Pract, 2020, 35(1):56-60. | |
| [37] | 计凤鸣, 王连敏, 丁珏宁君, 等. 胰腺实性假乳头状瘤的临床研究进展[J]. 医学综述, 2019, 25(5):909-914, 921. |
| JI F M, WANG L M, DING Y N J, et al. Progress in clinical research of solid pseudopapillary tumor of pancreas[J]. Med Recapitulate, 2019, 25(5):909-914, 921. | |
| [38] |
YU P, CHENG X, DU Y, et al. Solid pseudopapillary neoplasms of the pancreas: a 19-year multicenter experience in China[J]. J Gastrointest Surg, 2015, 19(8):1433-1440.
doi: 10.1007/s11605-015-2862-8 pmid: 26001371 |
| [39] |
YIN Q, WANG M, WANG C, et al. Differentiation between benign and malignant solid pseudopapillary tumor of the pancreas by MDCT[J]. Eur J Radiol, 2012, 81(11):3010-3018.
doi: 10.1016/j.ejrad.2012.03.013 pmid: 22520082 |
| [40] | VALSANGKAR N P, MORALES-OYARVIDE V, THAYER S P, et al. 851 resected cystic tumors of the pancreas: a 33-year experience at the Massachusetts General Hospital[J]. Surgery, 2012, 152(3 Suppl 1):S4-S12. |
| [41] | 张育森, 鲍世韵, 孙枫林, 等. 胰腺囊性肿瘤39例临床分析[J]. 中国医药导报, 2015(20):101-104. |
| ZHANG Y S, BAO S Y, SUN F L, et al. Clinical analysis of 39 cases with pancreatic cystic neoplasms[J]. Chin Med Herald, 2015, 12(20):101-104. | |
| [42] | CAGLIÀ P, CANNIZZARO M T, TRACIA A, et al. Cystic pancreatic neuroendocrine tumors: To date a diagnostic challenge[J]. Int J Surg, 2015, 21 Suppl 1:S44-S49. |
| [43] | 王慧, 李楠, 张艺璇, 等. 超声内镜下细针穿刺术对胰腺囊性神经内分泌肿瘤的诊断价值[J]. 中华胰腺病杂志, 2020, 20(5):386-388. |
| WANG H, LI N, ZHANG Y X, et al. The diagnostic value of EUS-FNA for pancreatic cystic neuroendocrine tumors[J]. Chin J Pancreatol, 2020, 20(5):386-388. | |
| [44] | KAWAMOTO S, JOHNSON P T, SHI C, et al. Pancreatic neuroendocrine tumor with cystlike changes: evaluation with MDCT[J]. Am J Roentgenol, 2013, 200(3):W283-W290. |
| [45] |
BAIOCCHI G L, PORTOLANI N, MISSALE G, et al. Intraductal papillary mucinous neoplasm of the pancreas (IPMN): clinico-pathological correlations and surgical indications[J]. World J Surg Oncol, 2010, 8:25.
doi: 10.1186/1477-7819-8-25 pmid: 20374620 |
| [1] | FENG Yuan, HE Zhao, SUN Qingfang, SUN Bomin, YAN Fuhua, YANG Guangzhong. Advances in interventional magnetic resonance imaging and its clinical applications [J]. Journal of Diagnostics Concepts & Practice, 2024, 23(02): 108-113. |
| [2] | ZHA Yunfei, WU Xiaxia. Application and research progress of MRI deep learning image reconstruction technology in clinical diagnosis of musculoskeletal system diseases [J]. Journal of Diagnostics Concepts & Practice, 2024, 23(02): 114-118. |
| [3] | LI Ming, CHEN Kemin, PAN Zilai, LUO Yu. Research progress on the value of CT and MRI in predicting hemorrhagic transformation after acute ischemic stroke [J]. Journal of Diagnostics Concepts & Practice, 2024, 23(01): 83-89. |
| [4] | DING Jingfeng, AO Weiqun, ZHU Zhen, SUN Jing, XU Lianggen, ZHENG Shibao, YU Jingjing, HU Jinwen. The value of radiomics based on T2WI and DWI of MRI in preoperative prediction of extramural vascular invasion in rectal cancer [J]. Journal of Diagnostics Concepts & Practice, 2024, 23(01): 46-56. |
| [5] | ZHOU Yilei, ZHANG Miao, GUO Rui, ZHOU Jinxin, LI Biao, LI Xiang. Value of 18F-PSMA PET/MRI for early diagnosis of recurrence and metastasis in prostate cancer patients after radical prostatectomy [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(06): 567-572. |
| [6] | FENG Li, REN Gang, CAI Rong, WANG Xinyun, WANG Hui, ZHU Mingjie. Clinical features study of perivascular epithelioid cell tumor (PEComa) in genitourinary system [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(05): 460-465. |
| [7] | DONG Lai, WANG Wei, WU Jialiang, LIU Yanpu, GUAN Xin, CHEN Kemin. Pulmonary imaging manifestations and related research progress of lymphangioleiomyomatosis [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(05): 501-506. |
| [8] | YIN Yongfang, TANG Yonghua, LIANG Yan, CHEN Zhiren, FEI Xiaochun. Clinical and imaging manifestations of Erdheim-Chester disease (six cases) [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(03): 283-291. |
| [9] | LI Xiaoshi, QIN Yue. Multiple radiology imaging techniques in the diagnosis of gout [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(03): 311-318. |
| [10] | CHEN Qian, LIN Huimin, YAN Fuhua. Advances in the evaluation of hepatic function by magnetic resonance imaging [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(02): 190-196. |
| [11] | YANG Wenjie, YAN Fuhua. Interpretation of the Clinical Practice Guidelines for Lung Cancer Screening (version 2) of 2022 National Comprehensive Cancer Network(NCCN) [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(01): 14-20. |
| [12] | HUANG Juan, ZHU Xiaolei, LI Xiao, CHEN Kemin, YAN Fuhua, XU Xueqin. Study on blood oxygen level-dependent magnetic resonance imaging for the assessment of early renal hypoxia in chronic kidney disease [J]. Journal of Diagnostics Concepts & Practice, 2022, 21(03): 385-389. |
| [13] | ZHU Naiyi, JIANG Yixin, CHAI Li, CHAI Weimin. Diagnostic values of magnetic resonance imaging in mammography detected BI-RADS≥4 category calcifications with negative ultrasound results [J]. Journal of Diagnostics Concepts & Practice, 2021, 20(05): 439-444. |
| [14] | ZHANG Xuekun, LI Yan, YAN Fuhua, ZHAO Hongfei, SONG Qi. Application value of new accelerating technology based on constellation shuttling imaging in brain MRI [J]. Journal of Diagnostics Concepts & Practice, 2021, 20(04): 378-383. |
| [15] | XU Hao, ZHANG Zhi, XIE Xueqian, YANG Wenyi, LIU Shaowen. Comparative study on software DEEPVESSEL FFR and invasive FFR in assessing coronary ischemia [J]. Journal of Diagnostics Concepts & Practice, 2021, 20(04): 384-390. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||